

Perioperative medication management: expanding the role of the preadmission clinic pharmacist in a single centre, randomised controlled trial of collaborative prescribing
- PMID: 23847268
- PMCID: PMC3710977
- DOI: 10.1136/bmjopen-2013-003027
Perioperative medication management: expanding the role of the preadmission clinic pharmacist in a single centre, randomised controlled trial of collaborative prescribing
Abstract
Objectives: Current evidence to support non-medical prescribing is predominantly qualitative, with little evaluation of accuracy, safety and appropriateness. Our aim was to evaluate a new model of service for the Australia healthcare system, of inpatient medication prescribing by a pharmacist in an elective surgery preadmission clinic (PAC) against usual care, using an endorsed performance framework.
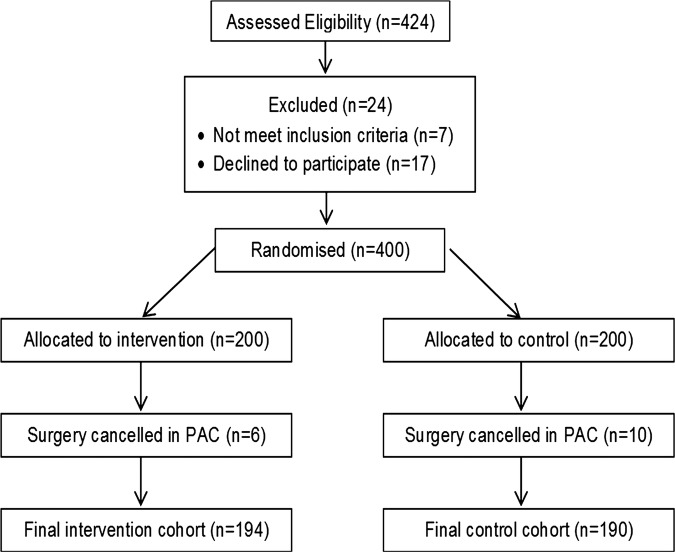
Design: Single centre, randomised controlled, two-arm trial.
Setting: Elective surgery PAC in a Brisbane-based tertiary hospital.
Participants: 400 adults scheduled for elective surgery were randomised to intervention or control.
Intervention: A pharmacist generated the inpatient medication chart to reflect the patient's regular medication, made a plan for medication perioperatively and prescribed venous thromboembolism (VTE) prophylaxis. In the control arm, the medication chart was generated by the Resident Medical Officers.
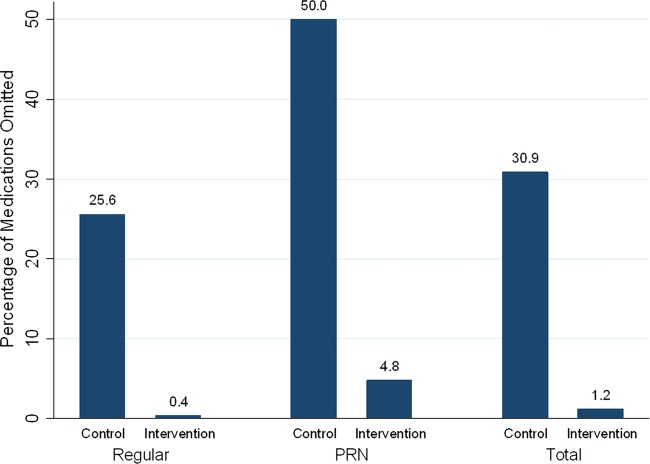
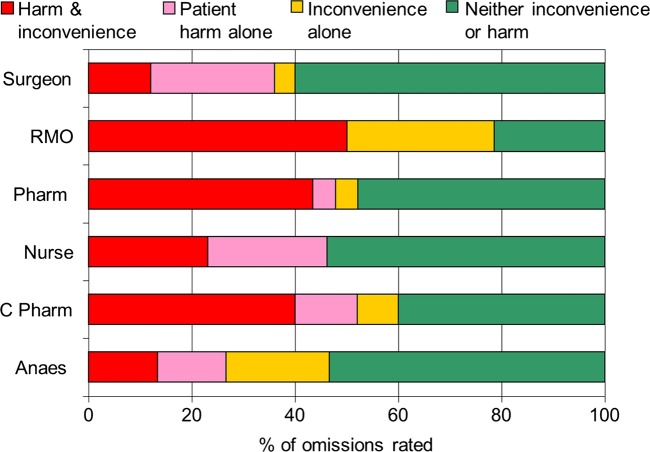
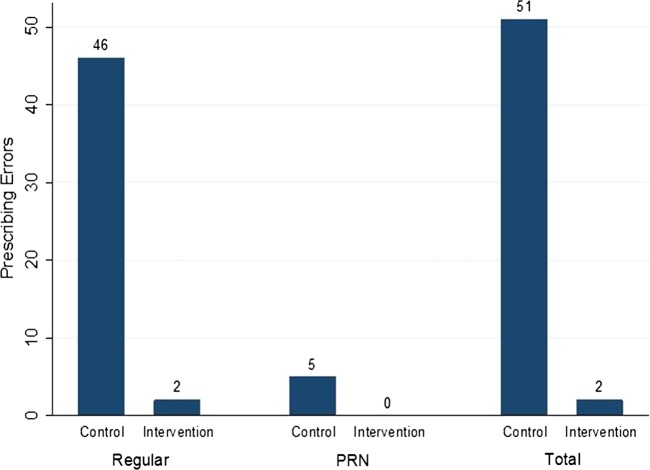
Outcome measures: Primary outcome was frequency of omissions and prescribing errors when compared against the medication history. The clinical significance of omissions was also analysed. Secondary outcome was appropriateness of VTE prophylaxis prescribing.
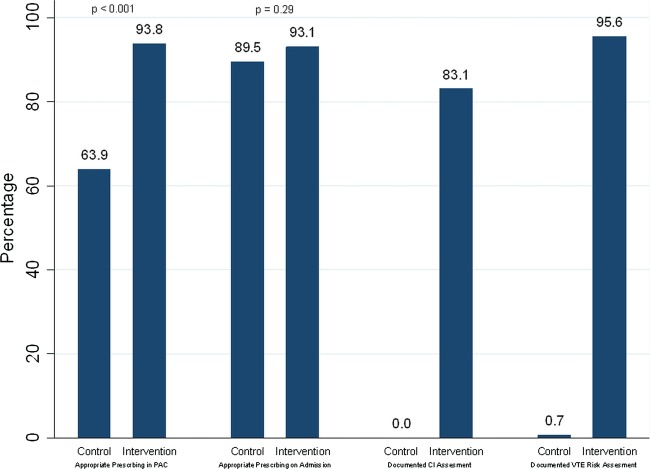
Results: There were significantly less unintended omissions of medications: 11 of 887 (1.2%) intervention orders compared with 383 of 1217 (31.5%) control (p<0.001). There were significantly less prescribing errors involving selection of drug, dose or frequency: 2 in 857 (0.2%) intervention orders compared with 51 in 807 (6.3%) control (p<0.001). Orders with at least one component of the prescription missing, incorrect or unclear occurred in 208 of 904 (23%) intervention orders and 445 of 1034 (43%) controls (p<0.001). VTE prophylaxis on admission to the ward was appropriate in 93% of intervention patients and 90% controls (p=0.29).
Conclusions: Medication charts in the intervention arm contained fewer clinically significant omissions, and prescribing errors, when compared with controls. There was no difference in appropriateness of VTE prophylaxis on admission between the two groups.
Trial registration: Registered with ANZCTR-ACTR Number ACTRN12609000426280.
Figures
References
-
- Bates D, Cullen D, Laird N, et al. Incidence of adverse drug events and potential adverse drug events: implications for prevention. JAMA 1995;274:29–34 - PubMed
-
- Bobb A, Gleason K, Husch M, et al. The epidemiology of prescribing errors: the potential impact of computerized prescriber order entry. Arch Intern Med 2004;164:785–92 - PubMed
-
- Cornish P, Knowles S, Marchesano R, et al. Unintended medication discrepancies at the time of hospital admission. Arch Intern Med 2005;165:424–9 - PubMed
-
- Bates D, Boyle D, Vander Villet M, et al. Relationship between medication errors and adverse drug events. J Gen Intern Med 1995;10:199–205 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources