

Ageism vs. the technical imperative, applying the GRADE framework to the evidence on hemodialysis in very elderly patients
- PMID: 23847412
- PMCID: PMC3700780
- DOI: 10.2147/CIA.S43817
Ageism vs. the technical imperative, applying the GRADE framework to the evidence on hemodialysis in very elderly patients
Abstract
Purpose: Treatment intensity for elderly patients with end-stage renal disease has escalated beyond population growth. Ageism seems to have given way to a powerful imperative to treat patients irrespective of age, prognosis, or functional status. Hemodialysis (HD) is a prime example of this trend. Recent articles have questioned this practice. This paper aims to identify existing pre-synthesized evidence on HD in the very elderly and frame it from the perspective of a clinician who needs to involve their patient in a treatment decision.
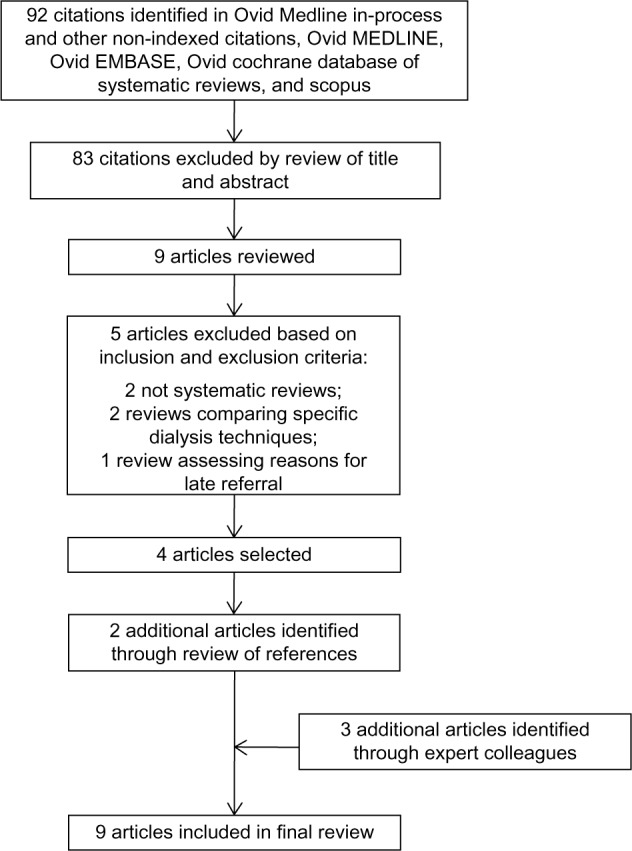
Patients and methods: A comprehensive search of several databases from January 2002 to August 2012 was conducted for systematic reviews of clinical and economic outcomes of HD in the elderly. We also contacted experts to identify additional references. We applied the rigorous framework of decisional factors of the Grading of Recommendation, Assessment, Development and Evaluation (GRADE) to evaluate the quality of evidence and strength of recommendations.
Results: We found nine eligible systematic reviews. The quality of the evidence to support the current recommendation of HD initiation for most very elderly patients is very low. There is significant uncertainty in the balance of benefits and risks, patient preference, and whether default HD in this patient population is a wise use of resources.
Conclusion: Following the GRADE framework, recommendation for HD in this population would be weak. This means it should not be considered standard of care and should only be started based on the well-informed patient's values and preferences. More studies are needed to delineate the true treatment effect and to guide future practice and policy.
Keywords: cost; quality of life; renal replacement therapy; resource utilization survival; symptom burden.
Figures
References
-
- Kurella M, Covinsky KE, Collins AJ, Chertow GM. Octogenarians and nonagenarians starting dialysis in the United States. Ann Intern Med. 2007;146(3):177–183. - PubMed
-
- Kjellstrand C. All elderly patients should be offered dialysis. Geriatr Nephrol Urol. 1997;6:129–136.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
