

Extension of the right internal thoracic artery with the radial artery in extensive re-do coronary artery bypass grafting
- PMID: 23849085
- PMCID: PMC3717112
- DOI: 10.1186/1749-8090-8-173
Extension of the right internal thoracic artery with the radial artery in extensive re-do coronary artery bypass grafting
Abstract
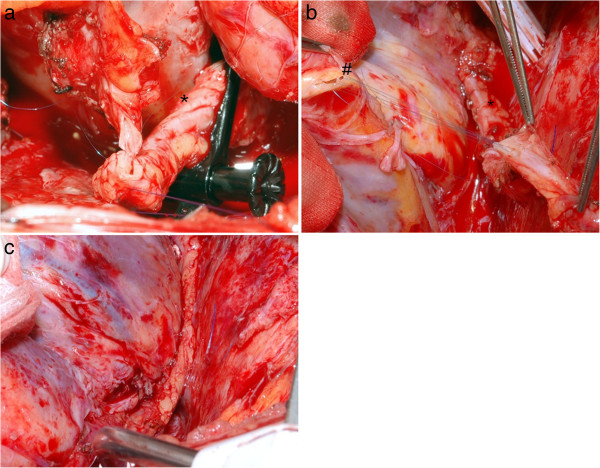
Background: Patients with extensive coronary artery disease often require re-do coronary artery bypass grafting. However, autologous bypass material is sometimes sparse. Since long term patency of arterial graft material is superior to venous bypass grafting, we developed a technique to perform re-do total arterial coronary artery bypass grafting extending the right internal thoracic artery (RITA) with the radial artery (RA) in an end to end fashion to gain the needed length in patients with and without an open left thoracic artery (LITA).
Methods: We performed this approach in 27 consecutive patients (age: 67.93 ± 7.51 years). Data was analyzed retrospectively. 19 operations were first re-op, 6 were second re-op and two were third re-op procedures.
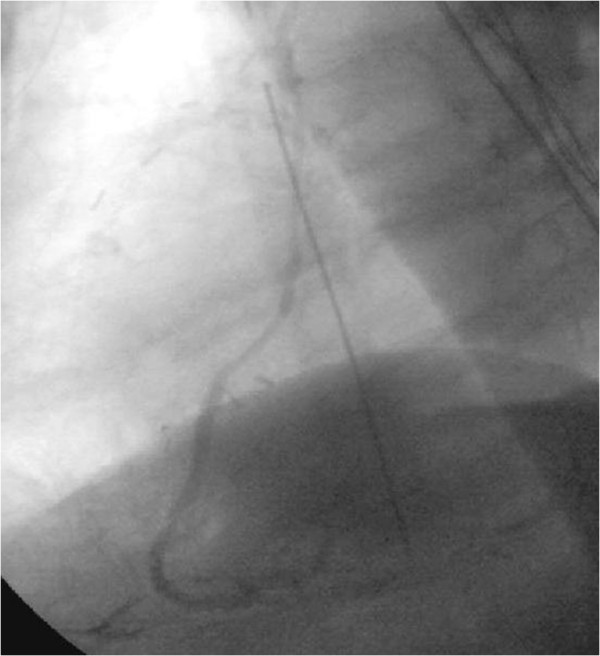
Results: Cardiopulmonary bypass time was 115.42 minutes (±31.92 minutes) with one OPCAB procedure, and clamp time was 55.09 minutes (±22.41 minutes) excluding 10 procedures performed on beating heart. Bypass grafting included the RCA, Cx and LAD. An average of 1.96 anastomoses were performed in each patient. Complication rate was low with one intra-operative apoplexy and one prolonged wound healing after harvest of the radial artery. One patient needed long term pulmonary assist. There was no intra-operative or early postoperative death.
Conclusion: The operational technique of elongation of the internal thoracic artery with the radial artery proved to be safe and feasible with acceptable operation times for a re-do procedure. We recommend this as an additional option to existing methods to perform a complete arterial revascularization mainly in patients with open left internal thoracic artery to LAD bypass.
Figures
Similar articles
-
The second best arterial graft: a propensity analysis of the radial artery versus the free right internal thoracic artery to bypass the circumflex coronary artery.J Thorac Cardiovasc Surg. 2014 Jan;147(1):133-40. doi: 10.1016/j.jtcvs.2013.08.040. Epub 2013 Oct 5. J Thorac Cardiovasc Surg. 2014. PMID: 24100104
-
Has the in situ right internal thoracic artery been overlooked? An angiographic study of the radial artery, internal thoracic arteries and saphenous vein graft patencies in symptomatic patients.Eur J Cardiothorac Surg. 2005 May;27(5):870-5. doi: 10.1016/j.ejcts.2005.01.027. Eur J Cardiothorac Surg. 2005. PMID: 15848328
-
Equipoise between radial artery and right internal thoracic artery as the second arterial conduit in left internal thoracic artery-based coronary artery bypass graft surgery: a multi-institutional study†.Eur J Cardiothorac Surg. 2016 Jan;49(1):188-95. doi: 10.1093/ejcts/ezv093. Epub 2015 Mar 11. Eur J Cardiothorac Surg. 2016. PMID: 25762396
-
Right internal thoracic or radial artery as the second arterial conduit for coronary artery bypass surgery.Curr Opin Cardiol. 2019 Sep;34(5):564-570. doi: 10.1097/HCO.0000000000000654. Curr Opin Cardiol. 2019. PMID: 31219879 Review.
-
Radial artery conduits for coronary artery bypass grafting: current perspective.J Thorac Cardiovasc Surg. 2005 Feb;129(2):250-3. doi: 10.1016/j.jtcvs.2004.07.040. J Thorac Cardiovasc Surg. 2005. PMID: 15678032 Review. No abstract available.
References
-
- Serruys PW, Morice MC, Kappetein AP, Colombo A, Holmes DR, Mack MJ, Ståhle E, Feldman TE, van den Brand M, Bass EJ, Van Dyck N, Leadley K, Dawkins KD, Mohr FW. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease. N Engl J Med. 2009;360(10):961–72. doi: 10.1056/NEJMoa0804626. - DOI - PubMed
-
- Cao C, Manganas C, Horton M, Bannon P, Munkholm-Larsen S, Ang SC, Yan TD. Angiographic outcomes of radial artery versus saphenous vein in coronary artery bypass graft surgery: A meta-analysis of randomized controlled trials. J Thorac Cardiovasc Surg. 2012;4 in press. - PubMed
-
- Salomon NW, Page US, Bigelow JC, Krause AH, Okies JE. M.T. Metzdorff Reoperative coronary surgery. Comparative analysis of 6591 patients undergoing primary bypass and 508 patients undergoing reoperative coronary artery bypass. J Thorac Cardiovasc Surg. 1990;100:250–259. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
