

Advanced imaging technologies increase detection of dysplasia and neoplasia in patients with Barrett's esophagus: a meta-analysis and systematic review
- PMID: 23851020
- PMCID: PMC3910269
- DOI: 10.1016/j.cgh.2013.06.017
Advanced imaging technologies increase detection of dysplasia and neoplasia in patients with Barrett's esophagus: a meta-analysis and systematic review
Abstract
Background & aims: US guidelines recommend surveillance of patients with Barrett's esophagus (BE) to detect dysplasia. BE conventionally is monitored via white-light endoscopy (WLE) and a collection of random biopsy specimens. However, this approach does not definitively or consistently detect areas of dysplasia. Advanced imaging technologies can increase the detection of dysplasia and cancer. We investigated whether these imaging technologies can increase the diagnostic yield for the detection of neoplasia in patients with BE, compared with WLE and analysis of random biopsy specimens.
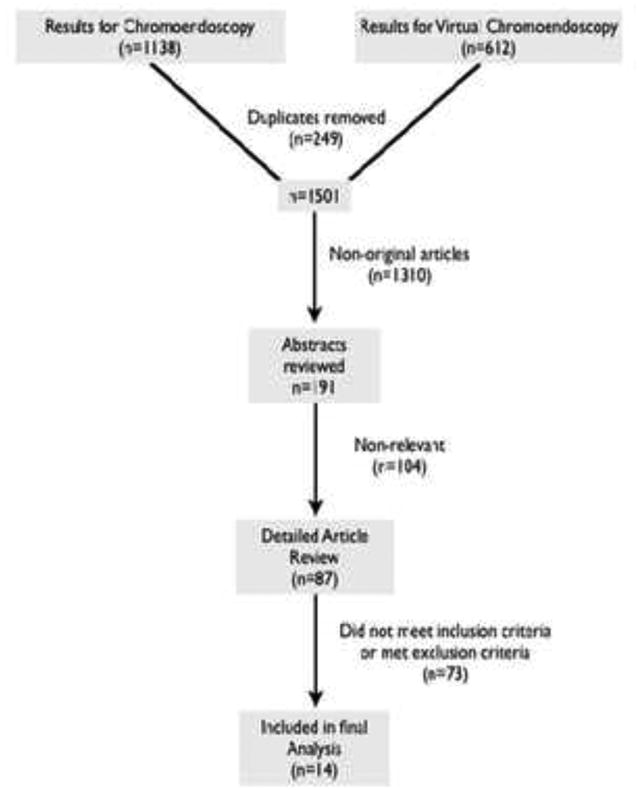
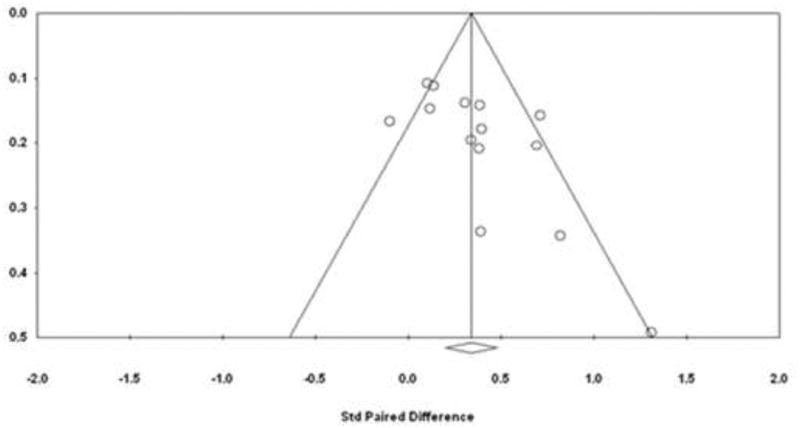
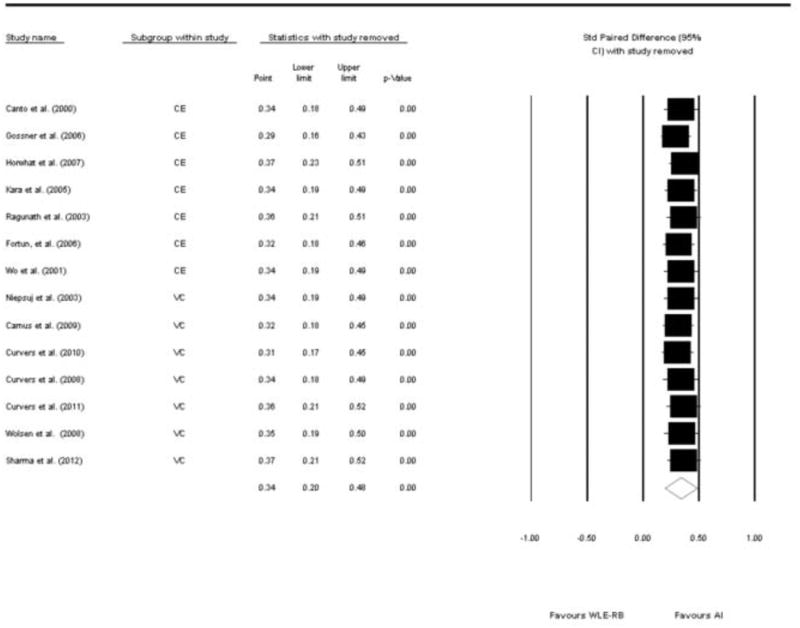
Methods: We performed a systematic review, using Medline and Embase, to identify relevant peer-review studies. Fourteen studies were included in the final analysis, with a total of 843 patients. Our metameter (estimate) of interest was the paired-risk difference (RD), defined as the difference in yield of the detection of dysplasia or cancer using advanced imaging vs WLE. The estimated paired-RD and 95% confidence interval (CI) were obtained using random-effects models. Heterogeneity was assessed by means of the Q statistic and the I(2) statistic. An exploratory meta-regression was performed to look for associations between the metameter and potential confounders or modifiers.
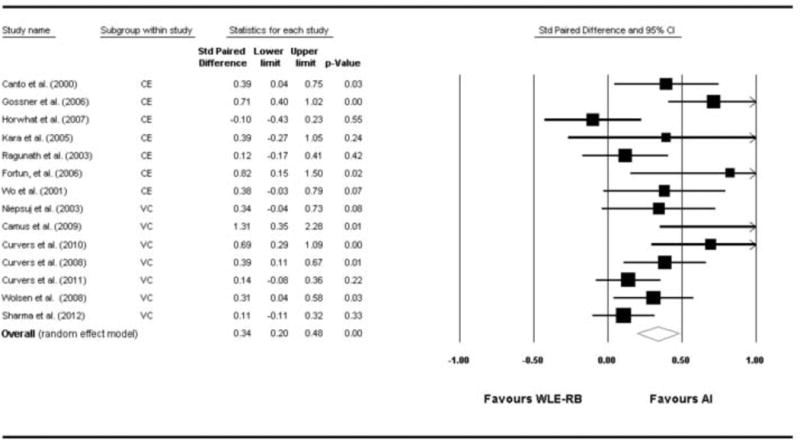
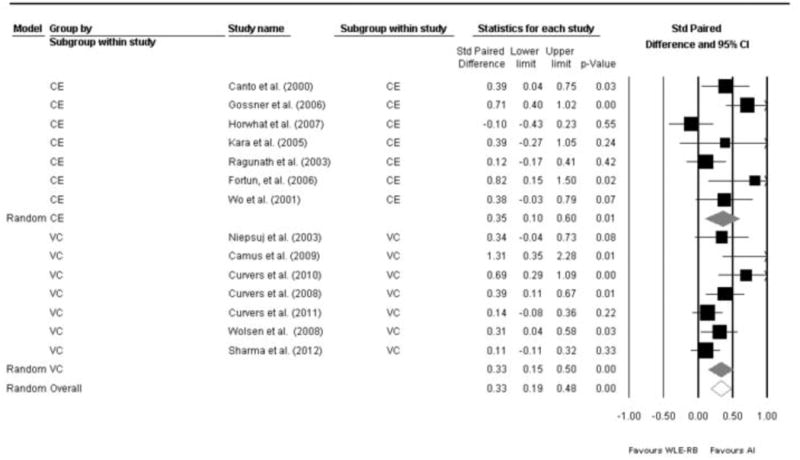
Results: Overall, advanced imaging techniques increased the diagnostic yield for detection of dysplasia or cancer by 34% (95% CI, 20%-56%; P < .0001). A subgroup analysis showed that virtual chromoendoscopy significantly increased the diagnostic yield (RD, 0.34; 95% CI, 0.14-0.56; P < .0001). The RD for chromoendoscopy was 0.35 (95% CI, 0.13-0.56; P = .0001). There was no significant difference between virtual chromoendoscopy and chromoendoscopy, based on Student t test analysis (P = .45).
Conclusions: Based on a meta-analysis, advanced imaging techniques such as chromoendoscopy or virtual chromoendoscopy significantly increase the diagnostic yield for identification of dysplasia or cancer in patients with BE.
Keywords: AI; Advanced Imaging; BE; Barrett’s Esophagus; Barrett’s esophagus; CBE; CE; CI; CLE; EAC; Esophageal Adenocarcinoma; FICE; Fujinon intelligent chromoendoscopy; NBI; PRISMA; QUADAS; Quality Assessment of Diagnostic Accuracy Studies; RB; RD; Risk Difference; VC; WLE; advanced imaging; chromoendoscopy; complete Barrett excision; confidence interval; confocal laser endomicroscopy; esophageal adenocarcinoma; narrow-band imaging; random biopsy; risk difference; virtual chromoendoscopy; white-light endoscopy.
Copyright © 2013 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Advanced imaging in Barrett's esophagus: are we ready to relinquish the random?Clin Gastroenterol Hepatol. 2013 Dec;11(12):1571-2. doi: 10.1016/j.cgh.2013.07.032. Epub 2013 Aug 4. Clin Gastroenterol Hepatol. 2013. PMID: 23924875 No abstract available.
References
-
- Rastogi A, Puli S, El-Serag HB, et al. Incidence of esophageal adenocarcinoma in patients with Barrett's esophagus and high-grade dysplasia: a meta-analysis. Gastrointest Endosc. 2008;67(3):394–8. Epub 2007/11/30. - PubMed
-
- Drewitz DJ, Sampliner RE, Garewal HS. The incidence of adenocarcinoma in Barrett's esophagus: a prospective study of 170 patients followed 4.8 years. Am J Gastroenterol. 1997;92(2):212–5. - PubMed
-
- Sharma P, Falk GW, Weston AP, et al. Dysplasia and cancer in a large multicenter cohort of patients with Barrett's esophagus. Clin Gastroenterol Hepatol. 2006;4(5):566–72. - PubMed
-
- Vizcaino AP, Moreno V, Lambert R, et al. Time trends incidence of both major histologic types of esophageal carcinomas in selected countries, 1973-1995. Int J Cancer. 2002;99(6):860–8. Epub 2002/07/13. - PubMed
-
- Pohl H, Welch HG. The role of overdiagnosis and reclassification in the marked increase of esophageal adenocarcinoma incidence. J Natl Cancer Inst. 2005;97(2):142–6. Epub 2005/01/20. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
