

Aortic valve replacement in geriatric patients with small aortic roots: are sutureless valves the future?
- PMID: 23851988
- PMCID: PMC3805192
- DOI: 10.1093/icvts/ivt291
Aortic valve replacement in geriatric patients with small aortic roots: are sutureless valves the future?
Abstract
Objectives: Aortic valve replacement (AVR) in geriatric patients (>75 years) with small aortic roots is a challenge. Patient-prosthesis mismatch and the long cross-clamp time necessary for stentless valves or root enlargement are matters of concern. We compared the results of AVR with sutureless valves (Sorin Perceval), against those with conventional biological valves.
Methods: Between April 2007 and December 2012, 120 isolated AVRs were performed in patients with a small annulus (<22 mm) at our centre. In 70 patients (68 females, age 77.4 ± 5.5 years), conventional valves (C group) and in 50 patients (47 females, age 79.8 ± 4.5 years), sutureless valves (P group) were implanted. The Logistic EuroSCORE of the C group was 16.7 ± 10.4 and that of the P group 20.4 ± 10.7, (P = 0.054). Minimal-access surgery was performed in 4.3% (3/70) patients in the C group and 72% (36/50) patients in the P group.
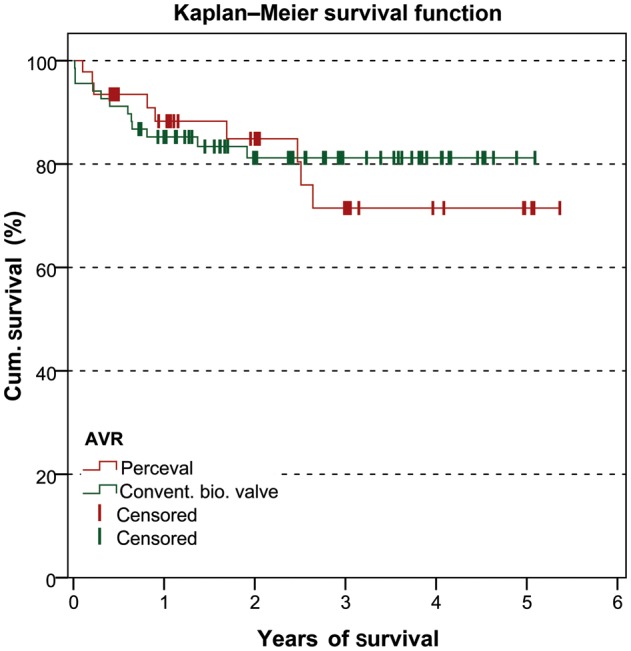
Results: The cardiopulmonary bypass (CPB) and cross-clamp times of the C group were 75.3 ± 23 and 50.3 ± 14.2 min vs 58.7 ± 20.9 and 30.1 ± 9 min in the P group, (P < 0.001). In the C group, two annulus enlargements were performed. Thirty-day mortality was 4.3% (n = 3) in the C group and 0 in the P group, (n.s.). At follow-up (up to 5 years), mortalities were 17.4% (n = 12) in the C group and 14% (n = 7) in the P group, (n.s.).
Conclusions: This study highlights the advantages of sutureless valves for geriatric patients with small aortic roots reflected by shorter cross-clamp and CPB times, even though most of these patients were operated on via a minimally invasive access. Moreover, due to the absence of a sewing ring, these valves are also almost stentless, with greater effective orifice area (EOA) for any given size. This may potentially result in better haemodynamics even without the root enlargement. This is of advantage, as several studies have shown that aortic root enlargement can significantly increase the risks of AVR. Moreover, as seen in this series, these valves may also enable a broader application of minimally invasive AVR.
Keywords: Aortic valve stenosis; Elderly patients; Small aortic root; Sutureless aortic valve.
Comment in
-
eComment. Incidence of patient-prosthesis mismatch in patients with a Perceval S valve.Interact Cardiovasc Thorac Surg. 2013 Nov;17(5):782-3. doi: 10.1093/icvts/ivt343. Interact Cardiovasc Thorac Surg. 2013. PMID: 24150047 Free PMC article. No abstract available.
References
-
- Rahimtoola SH. The problem of valve prosthesis-patient mismatch. Circulation. 1978;58:20–4. - PubMed
-
- Mohty D, Dumesnil JG, Echahidi N, Mathieu P. Impact of prosthesis-patient mismatch on long-term survival after aortic valve replacement: influence of age, obesity, and left ventricular dysfunction. J Am Coll Cardiol. 2009;53:39–47. - PubMed
-
- Blackstone EH, Cosgrove DM, Jamieson WR, Birkmeyer NJ, Lemmer JH, Miller DC, et al. Prosthesis size and long-term survival after aortic valve replacement. J Thorac Cardiovasc Surg. 2003;126:783–93. - PubMed
-
- Manouguian S, Seyblod-Epting W. Patch enlargement of the aortic valve ring by extending the aortic incision to the anterior mitral leaflet. J Thorac Cardiovasc Surg. 1979;78:402–12. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
