

FGF23 and mineral metabolism in the early post-renal transplantation period
- PMID: 23852336
- PMCID: PMC3796035
- DOI: 10.1007/s00467-013-2547-z
FGF23 and mineral metabolism in the early post-renal transplantation period
Abstract
Background: The relationship between fibroblast growth factor 23 (FGF23) and vitamin D production and catabolism post-renal transplantation has not been characterized.
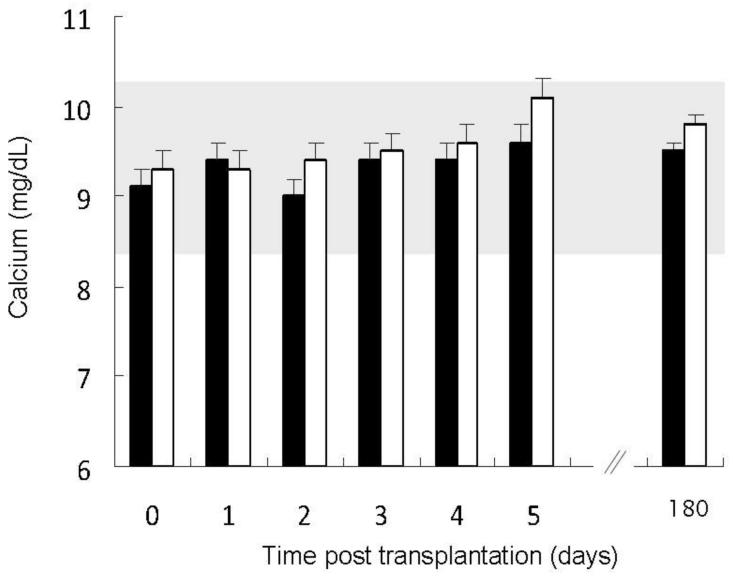
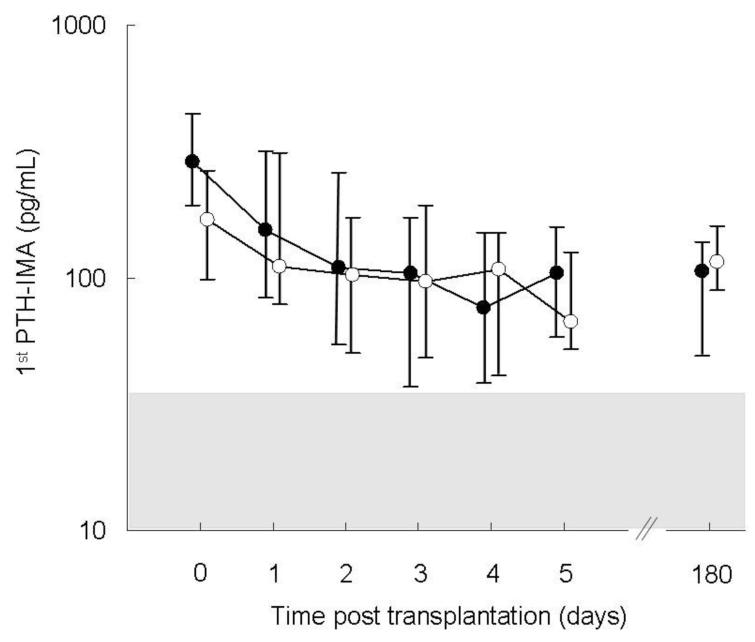
Methods: Circulating creatinine, calcium, phosphorus, albumin, parathyroid hormone, FGF23, and 1,25(OH)2 vitamin D (calcitriol) values were obtained pre-transplantation, daily post-operatively for 5 days, and at 6 months post-transplantation in 44 patients aged 16.4 ± 0.4 years undergoing renal transplantation at UCLA from 1 August 2005 through to 30 April 2007. 25(OH) Vitamin D and 24,25(OH)2 vitamin D concentrations were obtained at baseline and on post-operative days 5 and 180, and urinary concentrations of creatinine, phosphorus, and FGF23 were measured on post-operative days 1, 3, 5, and 180.
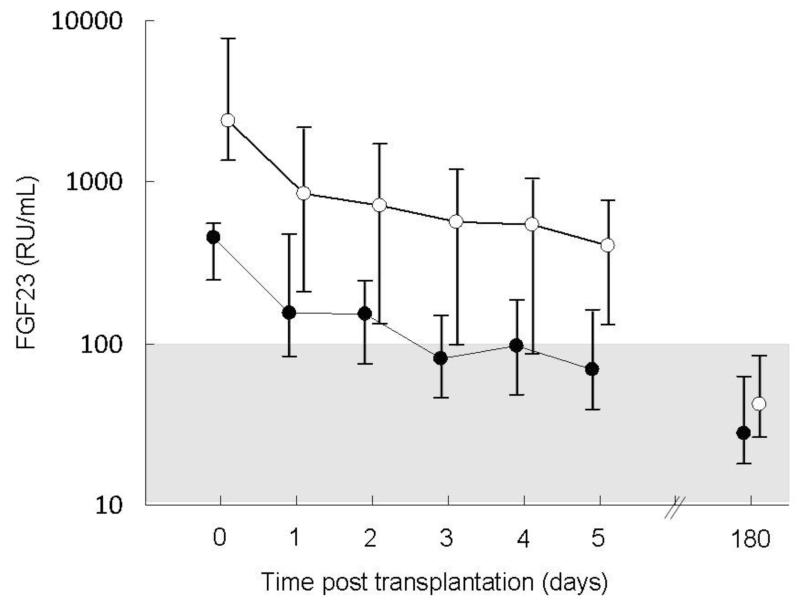
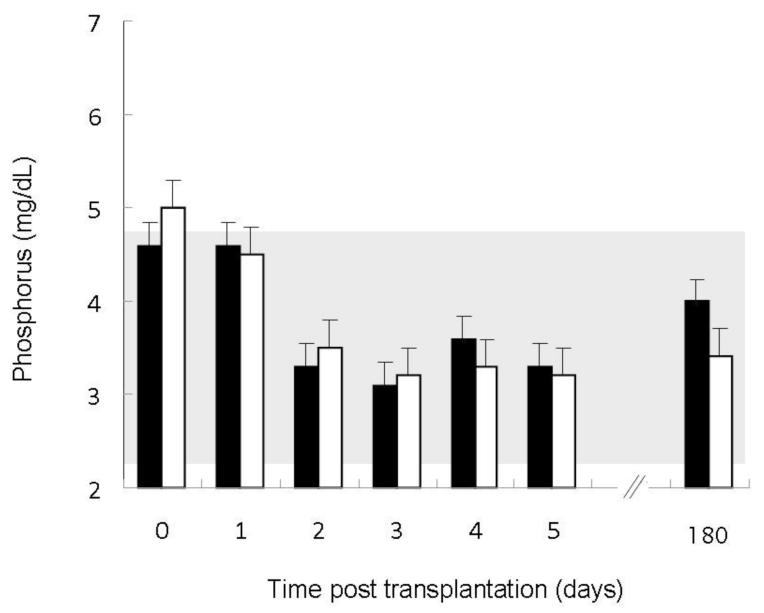
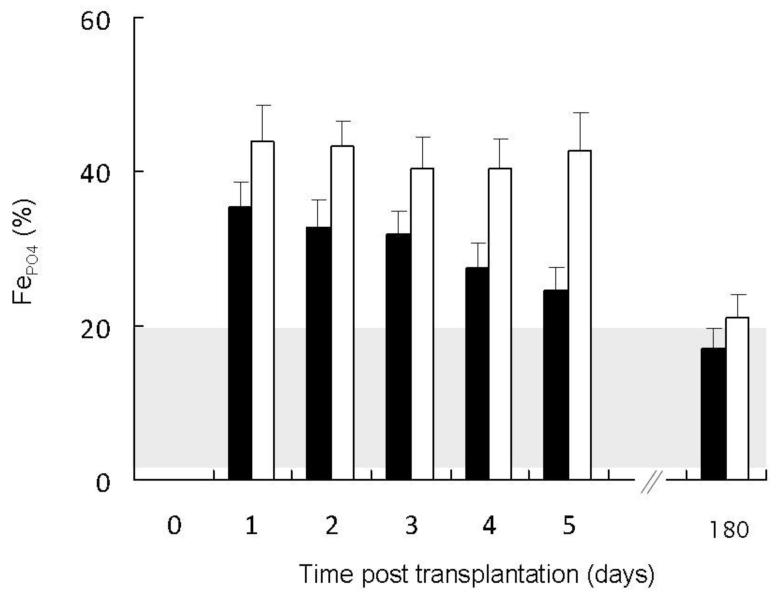
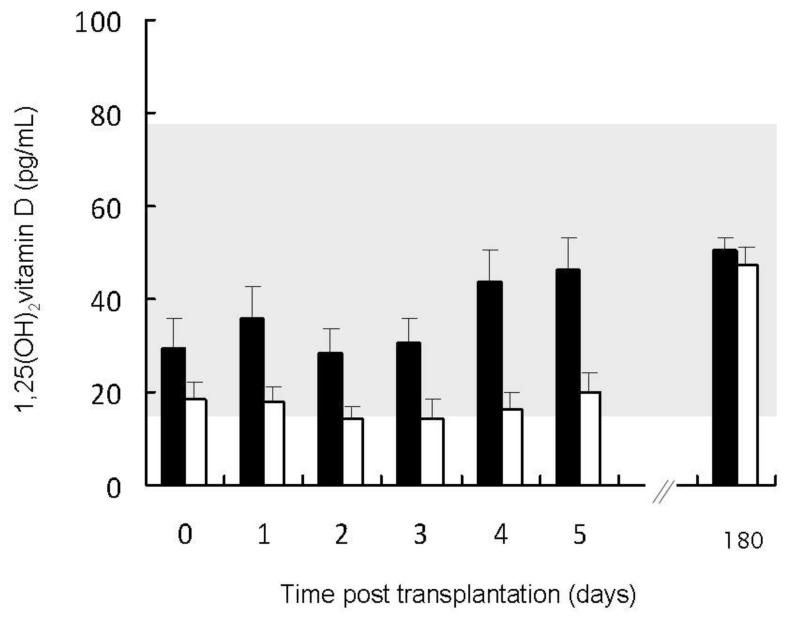
Results: Circulating phosphate concentrations declined more rapidly and the fractional excretion of phosphorus was higher in the first week post-transplantation in subjects with higher FGF23 values. Fractional excretion of FGF23 was low at all time-points. Circulating 1,25(OH)2 vitamin D levels rose more rapidly and were consistently higher in patients with lower FGF23 values; however, 25(OH) vitamin D and 24,25(OH)2 vitamin D values were unrelated to FGF23 concentrations.
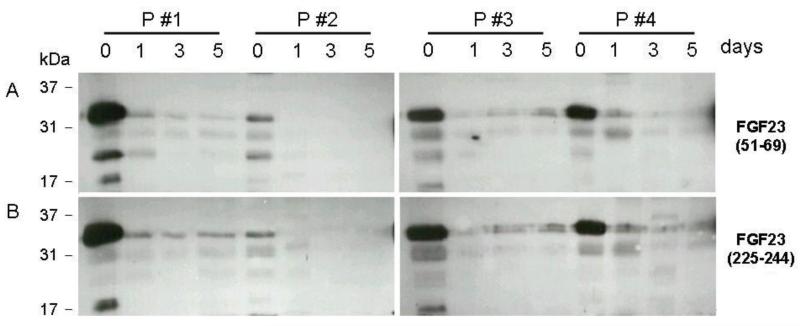
Conclusions: Inhibition of renal 1α-hydroxylase, rather than stimulation of 24-hydroxylase, may primarily contribute to the relationship between FGF23 values and calcitriol. The rapid decline in FGF23 levels post-transplantation in our patient cohort was not mediated solely by the filtration of intact FGF23 by the new kidney.
Figures
References
-
- Gutierrez O, Isakova T, Rhee E, Shah A, Holmes J, Collerone G, Jüppner H, Wolf M. Fibroblast growth factor-23 mitigates hyperphosphatemia but accentuates calcitriol deficiency in chronic kidney disease. J Am Soc Nephrol. 2005;16:2205–2215. - PubMed
-
- Fliser D, Kollerits B, Neyer U, Ankerst DP, Lhotta K, Lingenhel A, Ritz E, Kronenberg F, Kuen E, Konig P, Kraatz G, Mann JF, Muller GA, Kohler H, Riegler P. Fibroblast growth factor 23 (FGF23) predicts progression of chronic kidney disease: the Mild to Moderate Kidney Disease (MMKD) Study. J Am Soc Nephrol. 2007;18:2600–2608. - PubMed
-
- Isakova T, Xie H, Yang W, Xie D, Anderson AH, Scialla J, Wahl P, Gutierrez OM, Steigerwalt S, He J, Schwartz S, Lo J, Ojo A, Sondheimer J, Hsu CY, Lash J, Leonard M, Kusek JW, Feldman HI, Wolf M. Fibroblast growth factor 23 and risks of mortality and end-stage renal disease in patients with chronic kidney disease. JAMA. 2011;305:2432–2439. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- DK-080984/DK/NIDDK NIH HHS/United States
- DK-073039/DK/NIDDK NIH HHS/United States
- R01 DK035423/DK/NIDDK NIH HHS/United States
- UL1 TR000124/TR/NCATS NIH HHS/United States
- DK-67563/DK/NIDDK NIH HHS/United States
- DK-51081/DK/NIDDK NIH HHS/United States
- R01 DK073039/DK/NIDDK NIH HHS/United States
- DK-35423/DK/NIDDK NIH HHS/United States
- P01 DK011794/DK/NIDDK NIH HHS/United States
- R01 DK051081/DK/NIDDK NIH HHS/United States
- UL1 RR033176/RR/NCRR NIH HHS/United States
- P01 DK11794/DK/NIDDK NIH HHS/United States
- K23 DK080984/DK/NIDDK NIH HHS/United States
- UL1TR000124/TR/NCATS NIH HHS/United States
- UL1 RR-033176/RR/NCRR NIH HHS/United States
- R01 DK067563/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
