

Teriflunomide reduces relapse-related neurological sequelae, hospitalizations and steroid use
- PMID: 23852658
- PMCID: PMC3824843
- DOI: 10.1007/s00415-013-6979-y
Teriflunomide reduces relapse-related neurological sequelae, hospitalizations and steroid use
Abstract
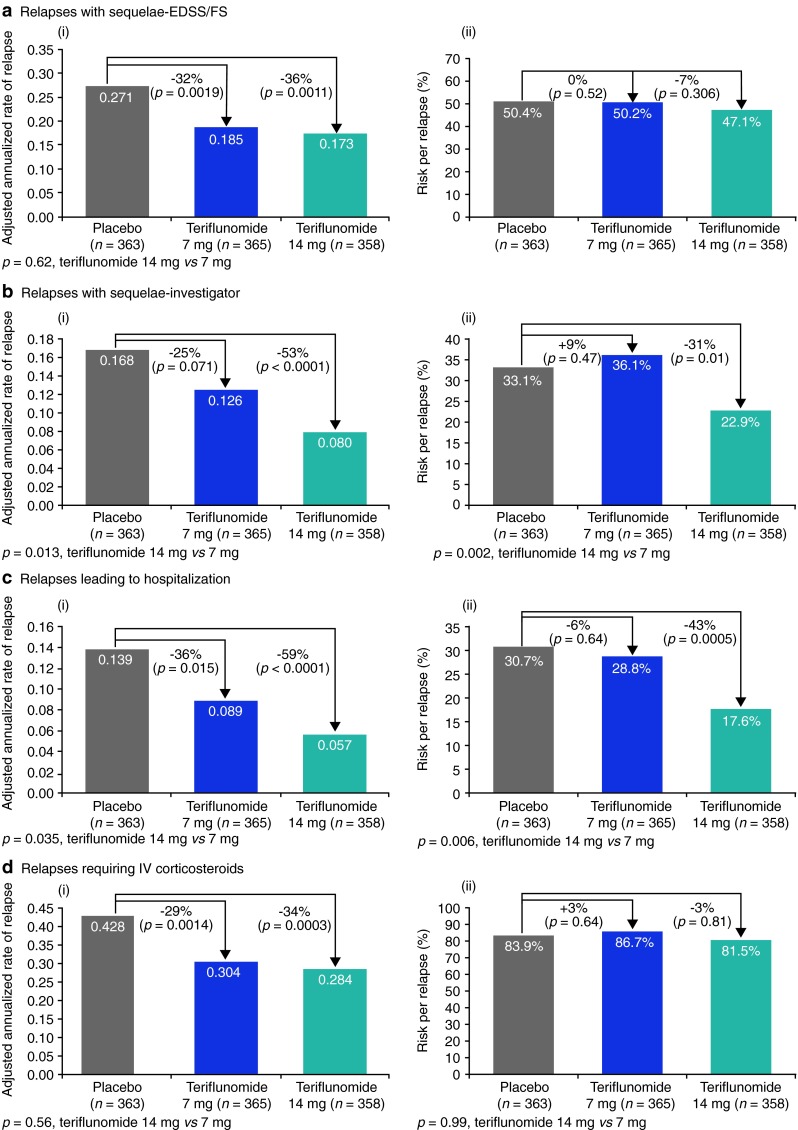
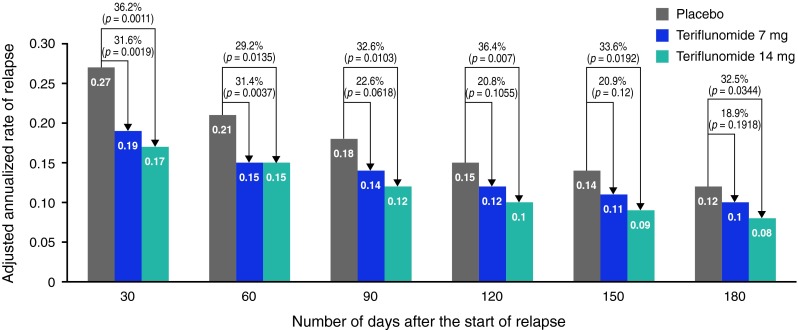
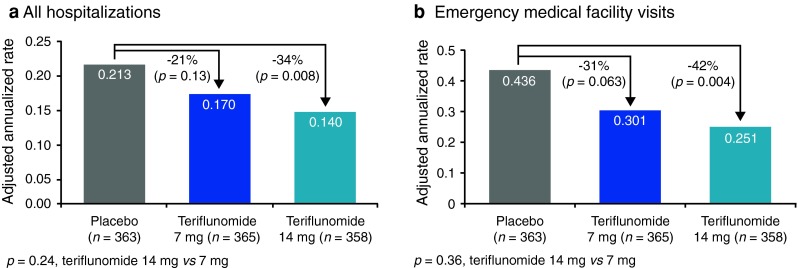
Multiple sclerosis (MS) relapses impose a substantial clinical and economic burden. Teriflunomide is a new oral disease-modifying therapy approved for the treatment of relapsing MS. We evaluated the effects of teriflunomide treatment on relapse-related neurological sequelae and healthcare resource use in a post hoc analysis of the Phase III TEMSO study. Confirmed relapses associated with neurological sequelae [defined by an increase in Expanded Disability Status Scale/Functional System (sequelae-EDSS/FS) ≥ 30 days post relapse or by the investigator (sequelae-investigator)] were analyzed in the modified intention-to-treat population (n = 1086). Relapses requiring hospitalization or intravenous (IV) corticosteroids, all hospitalizations, emergency medical facility visits (EMFV), and hospitalized nights for relapse were also assessed. Annualized rates were derived using a Poisson model with treatment, baseline EDSS strata, and region as covariates. Risks of sequelae and hospitalization per relapse were calculated as percentages and groups were compared with a χ(2) test. Compared with placebo, teriflunomide reduced annualized rates of relapses with sequelae-EDSS/FS [7 mg by 32 % (p = 0.0019); 14 mg by 36 % (p = 0.0011)] and sequelae-investigator [25 % (p = 0.071); 53 % (p < 0.0001)], relapses leading to hospitalization [36 % (p = 0.015); 59 % (p < 0.0001)], and relapses requiring IV corticosteroids [29 % (p = 0.001); 34 % (p = 0.0003)]. Teriflunomide-treated patients spent fewer nights in hospital for relapse (p < 0.01). Teriflunomide 14 mg also decreased annualized rates of all hospitalizations (p = 0.01) and EMFV (p = 0.004). The impact of teriflunomide on relapse-related neurological sequelae and relapses requiring healthcare resources may translate into reduced healthcare costs.
Figures
References
-
- Genzyme Corporation US LLC (2012) Aubagio® (teriflunomide) prescribing information
-
- Haas J, Hartung HP, von Rosenstiel P, Karlsson G, Tang D, Francis G, Kappos L, Cohen J (2011) Effect of fingolimod (FTY720) on severe multiple sclerosis relapses, healthcare utilization and recovery: results from two phase 3 studies, TRANSFORMS and FREEDOMS. Poster P06.049 presented at the 63rd Meeting of the American Academy of Neurology. Honolulu, Hawaii, USA, 9–16 April 2011
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
