

High-dose versus low-dose oxytocin for augmentation of delayed labour
- PMID: 23853046
- PMCID: PMC10575623
- DOI: 10.1002/14651858.CD007201.pub3
High-dose versus low-dose oxytocin for augmentation of delayed labour
Abstract
Background: A major cause of failure to achieve spontaneous vaginal birth is delay in labour due to presumed inefficient uterine action. Oxytocin is given to increase contractions and high-dose regimens may potentially increase the number of spontaneous vaginal births, but as oxytocin can cause hyperstimulation of the uterus, there is a possibility of increased adverse events.
Objectives: To compare starting dose and increment dose of oxytocin for augmentation for women delayed in labour to determine whether augmentation by high-dose regimens of oxytocin improves labour outcomes and to examine the effect on both maternal/neonatal outcomes and women's birth experiences.
Search methods: We searched the Cochrane Pregnancy and Childbirth Group's Trials Register (31 May 2013) and reference lists of retrieved studies.
Selection criteria: We included all randomised and quasi-randomised controlled trials for women in delayed labour requiring augmentation by oxytocin comparing high-dose regimens (defined as starting dose and increment of equal to or more than 4 mU per minute) with low-dose regimens (defined as starting dose and an increment of less than 4 mU per minute). Increase interval: between 15 and 40 minutes. The separation of low- and high-dose regimens is based on an arbitrary decision.
Data collection and analysis: Four review authors undertook assessment of trial eligibility, risk of bias, and data extraction independently.
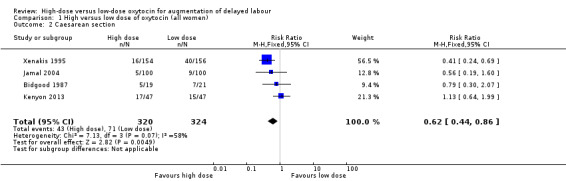
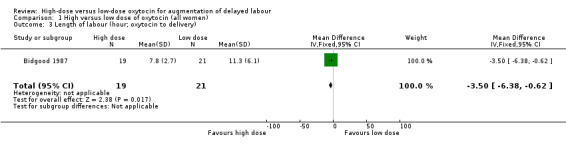
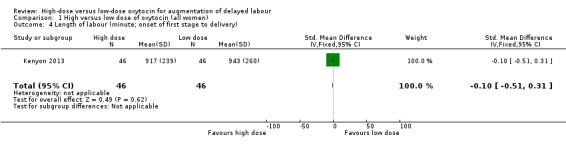
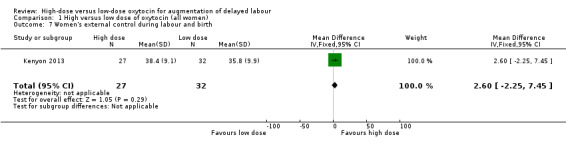
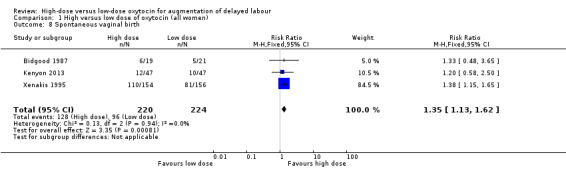
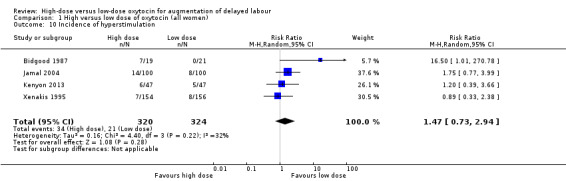
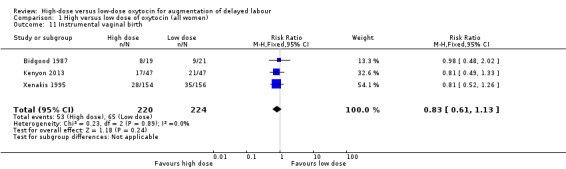
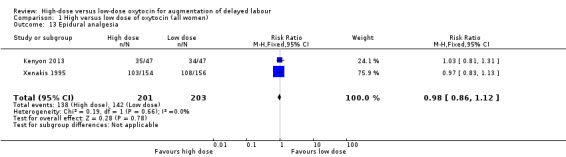
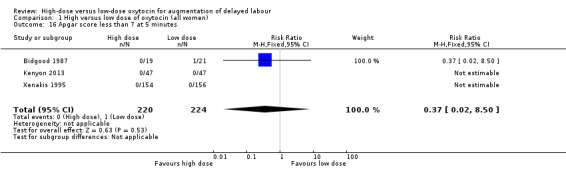
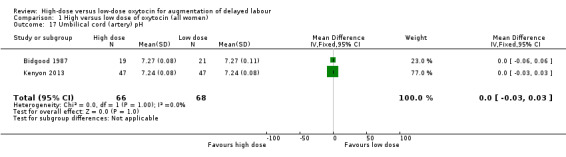
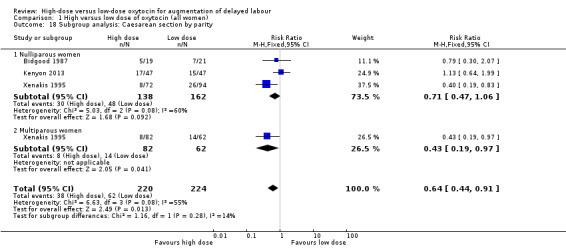
Main results: We included four studies involving 644 pregnant women. Three studies were randomised controlled trials and one trial was a quasi-randomised study. A higher dose of oxytocin was associated with a significant reduction in length of labour reported from one trial (mean difference (MD) -3.50 hours; 95% confidence interval (CI) -6.38 to -0.62; one trial, 40 women). There was a decrease in the rate of caesarean section (risk ratio (RR) 0.62; 95% CI 0.44 to 0.86 four trials, 644 women) and an increase in the rate of spontaneous vaginal birth in the high-dose group (RR 1.35; 95% CI 1.13 to 1.62, three trials, 444 women), although for both of these outcomes there were inconsistencies between studies in the size of effect. When we carried out sensitivity analysis (temporarily removing a study at high risk of bias) the differences between groups were no longer statistically significantThere were no significant differences between high- and low-dose regimens for instrumental vaginal birth, epidural analgesia, hyperstimulation, postpartum haemorrhage, chorioamnionitis or women's perceptions of experiences. For neonatal outcomes, there was no significant difference between groups for Apgar scores, umbilical cord pH, admission to special care baby unit, or neonatal mortality. The following outcomes were not evaluated in the included studies: perinatal mortality, uterine rupture, abnormal cardiotocography, women's pyrexia, dystocia and neonatal neurological morbidity.
Authors' conclusions: Higher-dose regimens of oxytocin (4 mU per minute or more) were associated with a reduction in the length of labour and in caesarean section, and an increase in spontaneous vaginal birth. However, there is insufficient evidence to recommend that high-dose regimens are advised routinely for women with delay in the first stage of labour. Further research should evaluate the effect of high-dose regimens of oxytocin for women delayed in labour and should include maternal and neonatal outcomes as well as the effects on women.
Conflict of interest statement
SK is the chief investigator of an included trial, and hence the trial was assessed by TD and RM independently. None known, otherwise.
Figures







Update of
-
High dose versus low dose oxytocin for augmentation of delayed labour.Cochrane Database Syst Rev. 2011 Oct 5;(10):CD007201. doi: 10.1002/14651858.CD007201.pub2. Cochrane Database Syst Rev. 2011. Update in: Cochrane Database Syst Rev. 2013 Jul 13;(7):CD007201. doi: 10.1002/14651858.CD007201.pub3. PMID: 21975767 Updated.
References
References to studies included in this review
Bidgood 1987 {published data only}
-
- Bidgood KA, Steer PJ. A randomized control study of oxytocin augmentation of labour. 1. Obstetric outcome. British Journal of Obstetrics and Gynaecology 1987;94:512‐7. - PubMed
-
- Bidgood KA, Steer PJ. A randomized control study of oxytocin augmentation of labour. 2. Uterine activity. British Journal of Obstetrics and Gynaecology 1987;94:518‐22. - PubMed
-
- Bidgood KA, Steer PJ. Oxytocin augmentation of labour. Proceedings of the 24th British Congress of Obstetrics and Gynaecology;1986 April 15‐18; Cardiff, UK. 1986:239.
Jamal 2004 {published data only}
-
- Jamal A, Kalantari R. High and low dose oxytocin in augmentation of labor. International Journal of Gynecology & Obstetrics 2004;87:6‐8. - PubMed
Kenyon 2013 {published data only}
-
- Bird D. High or low dose syntocinon (oxytocin) for delay in labour. Current Controlled Trials 2010.
Xenakis 1995 {published data only}
-
- Xenakis EM, Langer O, Piper JM, Conway D, Berkus MD. Low‐dose versus high‐dose oxytocin augmentation of labor‐‐a randomized trial. American Journal of Obstetrics and Gynecology 1995;173:1874‐8. - PubMed
-
- Xenakis EMJ, Field N, Barshes D, Langer O. Efficacy of high dose vs low dose oxytocin in labor augmentation. American Journal of Obstetrics and Gynecology 1994;170:378.
References to studies excluded from this review
Akoury 1993 {published data only}
-
- Akoury H, Brodie G, Caddick R, Chandbry N, Pugh N, Rowell Y. Oxytocin augmentation of labour: a comparison between high and low dose protocol and perinatal outcome a nulliparous women. Proceedings of 49th Annual Clinical Meeting of the Society of Obstetricians and Gynaecologists of Canada; 1993 June 22‐26; Ottawa, Ontario, Canada. 1993:14.
Alderman 1974 {published data only}
Arulkumaran 1989 {published data only}
-
- Arulkumaran S, Yang M, Ingemarsson I, Singh P, Ratnam SS. Augmentation of labour: does oxytocin titration to achieve preset active contraction area values produce better obstetric outcome?. Asia‐Oceania Journal of Obstetrics and Gynaecology 1989;15:333‐7. - PubMed
Cummiskey 1989 {published data only}
-
- Cummiskey KC, Gall SA, Yusoff DM. Pulsatile administration of oxytocin for augmentation of labor. Obstetrics & Gynecology 1989;74(6):869‐72. - PubMed
Doppa 2011 {published data only}
-
- Doppa GJ. Low dose vs high dose oxytocin in augmentation of labour in KVGMC. Clinical Trials Registry ‐ India 2011.
Hayakungchat 2011 {published data only}
-
- Swadpanich US. The effects of high versus low dose oxytocin on cesarean section rate, fetal and maternal outcomes for augmentation of labor in pregnant women gestational age > 37 weeks. Australian New Zealand Clinical Trials Registry (www.anzctr.org.au) 2011.
Lazor 1993 {published data only}
-
- Lazor LZ, Philipson EH, Ingardia CJ, Kobetitsch ES, Curry SL. A randomized comparison of 15‐ and 40‐minute dosing protocols for labor augmentation and induction. Obstetrics & Gynecology 1993;82:1009‐12. - PubMed
-
- Lazor LZ, Philipson EH, Ingardia CJ, Kobetitsch ES, Curry SL. A randomized prospective comparison of oxytocin dosing protocols for labor augmentation in nulliparous women. American Journal of Obstetrics and Gynecology 1993;168:295. - PubMed
Lowensohn 1990 {published data only}
-
- Lowensohn RI, Jensen JT. Oxytocin use in induction and augmentation of labor. Proceedings of 10th Annual Meeting of Society of Perinatal Obstetricians; 1990 January 23‐27; Houston, Texas, USA. 1991:76.
Majoko 2001 {published data only}
-
- Majoko F. Effectiveness and safety of high dose oxytocin for augmentation of labour in nulliparous women. Central African Journal of Medicine 2001;47(11‐12):247‐50. - PubMed
Merrill 1999 {published data only}
-
- Merrill DC, Zlatnik FJ. Randomized, double‐masked comparison of oxytocin dosage in induction and augmentation of labor. Obstetrics & Gynecology 1999;94:455‐63. - PubMed
Parpas 1995 {published data only}
-
- Parpas G, Gondry J, Verhoest P, Martinez C, Boulanger JCh. Randomised trial of 2 dosages of oxytocin for labour induction or augmentation [Utilisation de l'ocytocine (syntocinon) dans le declenchement ou la direction du travail: faible ou forte posologie, comparaison]. Journal de Gynecologie, Obstetrique et Biologie de la Reproduction 1995;24(8):873.
Satin 1994 {published data only}
-
- Satin AJ, Leveno KJ, Sherman L, McIntire D. High‐dose oxytocin: 20‐ versus 40‐minute dosage interval. Obstetrics & Gynecology 1994;83(2):238. - PubMed
Seitchik 1982 {published data only}
-
- Seitchik J, Castillo M. Oxytocin augmentation of dysfunctional labor? I. Clinical data. American Journal of Obstetrics and Gynecology 1982;144:899‐905. - PubMed
Supajitkulchi 2003 {published data only}
-
- Supajitkulchi S, Sritongchai C. A comparison of high and low oxytocin concentration in active phase of labor. Chon Buri Hospital Journal 2003;28(1):11‐5.
Vorherr 1963 {published data only}
-
- Vorherr H. Is there a pharmacological acceleration of childbirth? [Gibt es eine medikamentose Geburtsbeschleunigung?]. Deutsche Medizinische Wochenschrift 1963;88:1426‐30. - PubMed
References to ongoing studies
Berg 2012 {published data only}
-
- Berg M. High dose versus low dose oxytocin for augmentation of delayed labour. ClinicalTrials.gov 2012.
Additional references
Deeks 2001
-
- Deeks JJ, Altman DG, Bradburn MJ. Statistical methods for examining heterogeneity and combining results from several studies in meta‐analysis. In: Egger M, Davey Smith G, Altman DG editor(s). Systematic Reviews in Health Care: Meta‐Analysis in Context. London: BMJ Books, 2001.
DOH 2004
-
- Government Statistical Service for the Department of Health. NHS Maternity Statistics. London: Department of Health, 2004.
Egger 1997
Ford 2009
-
- Ford E, Ayers S. Measurement of maternal perceptions of Support and Control in Birth (SCIB). Journal of Women's Health 2009;18:245‐52. - PubMed
Gottschall 1997
-
- Gottschall DS, Borgida AF, Mihalek JJ, Sauer F, Rodis JF. A randomized clinical trial comparing misoprostol with prostaglandin E2 gel for preinduction cervical ripening. American Journal of Obstetrics and Gynecology 1997;177(5):1067‐70. - PubMed
Harbord 2006
-
- Harbord RM, Egger M, Sterne JA. A modified test for small‐study effects in meta‐analyses of controlled trials with binary endpoints. Statistics in Medicine 2006;25(20):3443‐57. - PubMed
Higgins 2011
-
- Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Impey 2000
-
- Impey L, Hobson J, O'Herlihy C. Graphic analysis of actively managed labor: prospective computation of labor progress in 500 consecutive nulliparous women in spontaneous labor at term. American Journal of Obstetrics and Gynecology 2000;183(2):438‐43. - PubMed
NICE 2007
-
- National Collaborating Centre for Women's and Children's Health. Intrapartum Care: Care of Healthy Women and Their Babies During Childbirth. London: RCOG Press 2007. - PubMed
RevMan 2012 [Computer program]
-
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.2. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2012.
Smyth 2007
Wei 2007
-
- Wei SQ, Wo BL, Xu HR, Roy C, Turcot L, Fraser WD. Early amniotomy and early oxytocin for delay in first stage spontaneous labor compared with routine care. Cochrane Database of Systematic Reviews 2007, Issue 4. [DOI: 10.1002/14651858.CD006794] - DOI
Wei 2010
-
- Wei SQ, Luo ZC, Qi HP, Xu H, Fraser WD. High‐dose vs low‐dose oxytocin for labor augmentation: a systematic review. American Journal of Obstetrics and Gynecology 2010;203:296‐304. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials