

Strength Training for Arthritis Trial (START): design and rationale
- PMID: 23855596
- PMCID: PMC3722013
- DOI: 10.1186/1471-2474-14-208
Strength Training for Arthritis Trial (START): design and rationale
Abstract
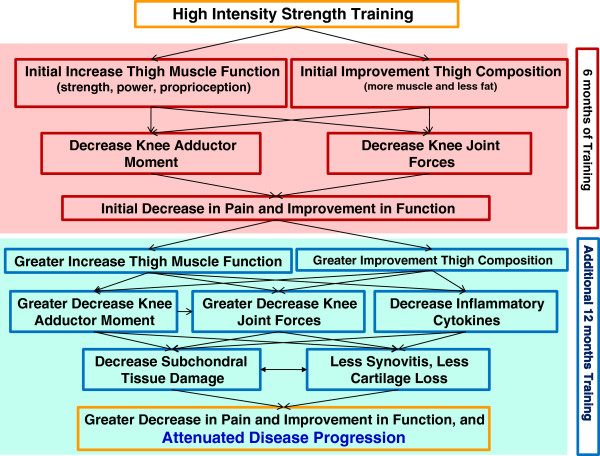
Background: Muscle loss and fat gain contribute to the disability, pain, and morbidity associated with knee osteoarthritis (OA), and thigh muscle weakness is an independent and modifiable risk factor for it. However, while all published treatment guidelines recommend muscle strengthening exercise to combat loss of muscle mass and strength in knee OA patients, previous strength training studies either used intensities or loads below recommended levels for healthy adults or were generally short, lasting only 6 to 24 weeks. The efficacy of high-intensity strength training in improving OA symptoms, slowing progression, and affecting the underlying mechanisms has not been examined due to the unsubstantiated belief that it might exacerbate symptoms. We hypothesize that in addition to short-term clinical benefits, combining greater duration with high-intensity strength training will alter thigh composition sufficiently to attain long-term reductions in knee-joint forces, lower pain levels, decrease inflammatory cytokines, and slow OA progression.
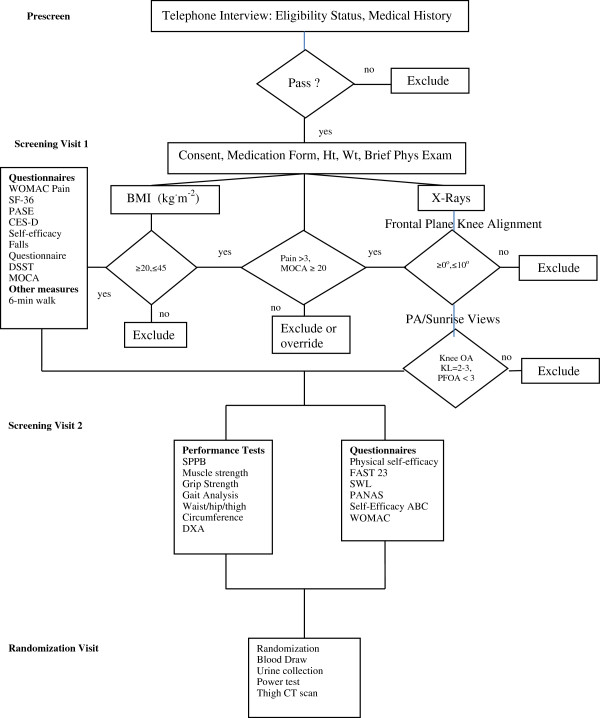
Methods/design: This is an assessor-blind, randomized controlled trial. The study population consists of 372 older (age ≥ 55 yrs) ambulatory, community-dwelling persons with: (1) mild-to-moderate medial tibiofemoral OA (Kellgren-Lawrence (KL) = 2 or 3); (2) knee neutral or varus aligned knee ( -2° valgus ≤ angle ≤ 10° varus); (3) 20 kg.m-2 ≥ BMI ≤ 45 kg.m-2; and (3) no participation in a formal strength-training program for more than 30 minutes per week within the past 6 months. Participants are randomized to one of 3 groups: high-intensity strength training (75-90% 1Repetition Maximum (1RM)); low-intensity strength training (30-40%1RM); or healthy living education. The primary clinical aim is to compare the interventions' effects on knee pain, and the primary mechanistic aim is to compare their effects on knee-joint compressive forces during walking, a mechanism that affects the OA disease pathway. Secondary aims will compare the interventions' effects on additional clinical measures of disease severity (e.g., function, mobility); disease progression measured by x-ray; thigh muscle and fat volume, measured by computed tomography (CT); components of thigh muscle function, including hip abductor strength and quadriceps strength, and power; additional measures of knee-joint loading; inflammatory and OA biomarkers; and health-related quality of life.
Discussion: Test-retest reliability for the thigh CT scan was: total thigh volume, intra-class correlation coefficients (ICC) = 0.99; total fat volume, ICC = 0.99, and total muscle volume, ICC = 0.99. ICC for both isokinetic concentric knee flexion and extension strength was 0.93, and for hip-abductor concentric strength was 0.99. The reliability of our 1RM testing was: leg press, ICC = 0.95; leg curl, ICC = 0.99; and leg extension, ICC = 0.98. Results of this trial will provide critically needed guidance for clinicians in a variety of health professions who prescribe and oversee treatment and prevention of OA-related complications. Given the prevalence and impact of OA and the widespread availability of this intervention, assessing the efficacy of optimal strength training has the potential for immediate and vital clinical impact.
Trial registration: ClinicalTrials.gov, NCT01489462.
Figures
References
-
- Hootman JM, Fitzgerald SJ, Macera CA, Blair SN. Lower extremity muscle strength and risk of self-reported hip or knee osteoarthritis. Journal of Physical Activity and Health. 2004;1:321–330.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
