

Phase II trial of neoadjuvant bevacizumab plus chemotherapy and adjuvant bevacizumab in patients with resectable nonsquamous non-small-cell lung cancers
- PMID: 23857398
- PMCID: PMC4191830
- DOI: 10.1097/JTO.0b013e31829923ec
Phase II trial of neoadjuvant bevacizumab plus chemotherapy and adjuvant bevacizumab in patients with resectable nonsquamous non-small-cell lung cancers
Abstract
Introduction: Bevacizumab improves survival in patients with advanced non-small-cell lung cancer (NSCLC). This phase II clinical trial assessed the effects of the addition of bevacizumab to neoadjuvant chemotherapy in resectable nonsquamous NSCLC.
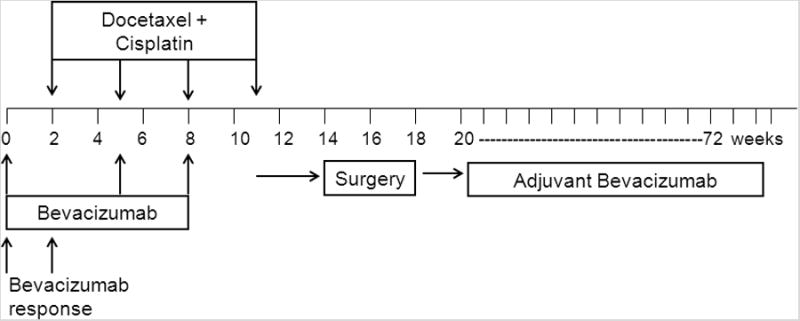
Methods: Patients with resectable stage IB-IIIA nonsquamous NSCLC were treated with bevacizumab followed by imaging 2 weeks later to assess single-agent effect. After this they received two cycles of bevacizumab with four cycles of cisplatin and docetaxel followed by surgical resection. Resected patients were eligible for adjuvant bevacizumab. The primary endpoint was the rate of pathological downstaging (decrease from pretreatment clinical stage to post-treatment pathological stage). Secondary endpoints included overall survival, safety, and radiologic response.
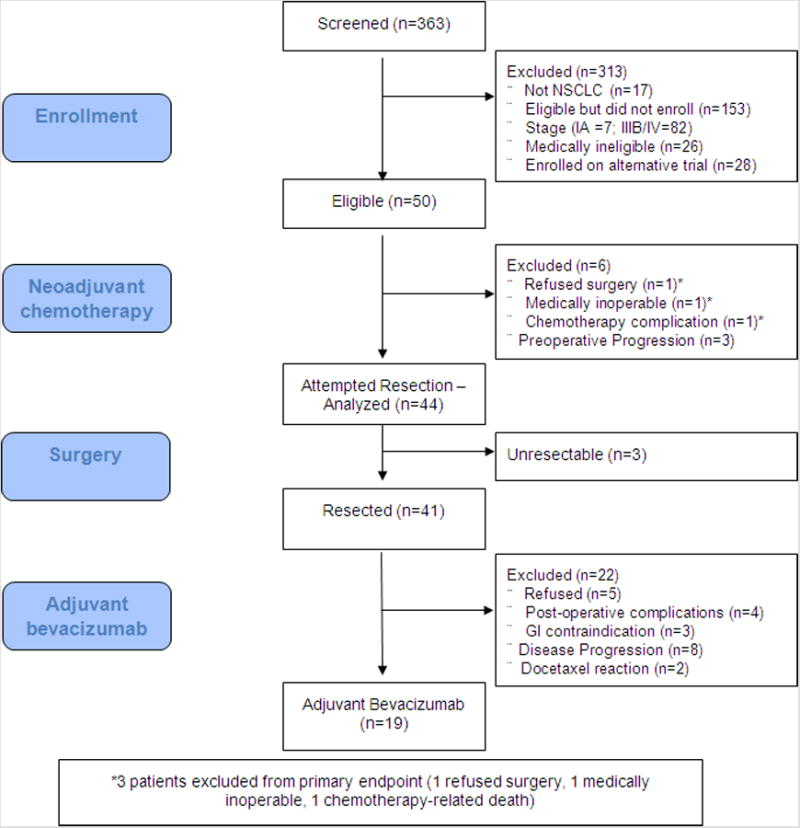
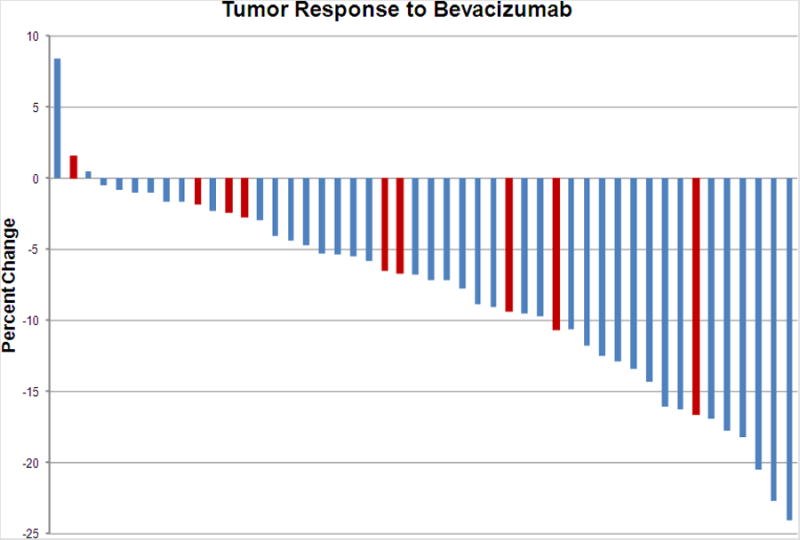
Results: Fifty patients were enrolled. Thirty-four (68%) were clinical stage IIIA. All three doses of neoadjuvant bevacizumab were delivered to 40 of 50 patients. Six patients (12%) discontinued because of bevacizumab-related adverse events. The rate of downstaging (38%), response to chemotherapy (45%), and perioperative complications (12%) were comparable with historical data. No partial responses were observed to single-agent bevacizumab, but 18% of the patients developed new intratumoral cavitation, with a trend toward improved pathologic response (57% versus 21%; p = 0.07). A major pathologic response (≥90% treatment effect) was associated with survival at 3 years (100% versus 49%; p = 0.01). No patients with KRAS-mutant NSCLC (0 of 10) had a pathologic response as compared with 11 of 31 with wild-type KRAS.
Conclusion: Although preoperative bevacizumab plus chemotherapy was feasible, it did not improve downstaging in unselected patients. New cavitation after single-agent bevacizumab is a potential biomarker. Alternative strategies are needed for KRAS-mutant tumors.
Figures
References
-
- Douillard JY, Tribodet H, Aubert D, et al. Adjuvant cisplatin and vinorelbine for completely resected non-small cell lung cancer: subgroup analysis of the Lung Adjuvant Cisplatin Evaluation. J Thorac Oncol. 2010;5:220–228. - PubMed
-
- Felip E, Massuti B, Alonso G, et al. Surgery Alone, or Surgery Followed by Adjuvant Paclitaxel/Carboplatin (PC) or Preoperative PC Followed by Surgery, in Early Stage Non-Small Cell Lung Cancer: Results of the Multicenter, Randomized, Phase III NATCH Trial. J Clin Oncol. 2009;(27):CRA7500.
-
- Betticher DC, Hsu Schmitz SF, Totsch M, et al. Mediastinal lymph node clearance after docetaxel-cisplatin neoadjuvant chemotherapy is prognostic of survival in patients with stage IIIA pN2 non-small-cell lung cancer: a multicenter phase II trial. J Clin Oncol. 2003;21:1752–1759. - PubMed
-
- Dooms C, Verbeken E, Stroobants S, et al. Prognostic stratification of stage IIIA-N2 non-small-cell lung cancer after induction chemotherapy: a model based on the combination of morphometric-pathologic response in mediastinal nodes and primary tumor response on serial 18-fluoro-2-deoxy-glucose positron emission tomography. J Clin Oncol. 2008;26:1128–1134. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
