

Mechanical ventilation and acute lung injury in emergency department patients with severe sepsis and septic shock: an observational study
- PMID: 23859579
- PMCID: PMC3718493
- DOI: 10.1111/acem.12167
Mechanical ventilation and acute lung injury in emergency department patients with severe sepsis and septic shock: an observational study
Abstract
Objectives: The objectives were to characterize the use of mechanical ventilation in the emergency department (ED), with respect to ventilator settings, monitoring, and titration and to determine the incidence of progression to acute lung injury (ALI) after admission, examining the influence of factors present in the ED on ALI progression.
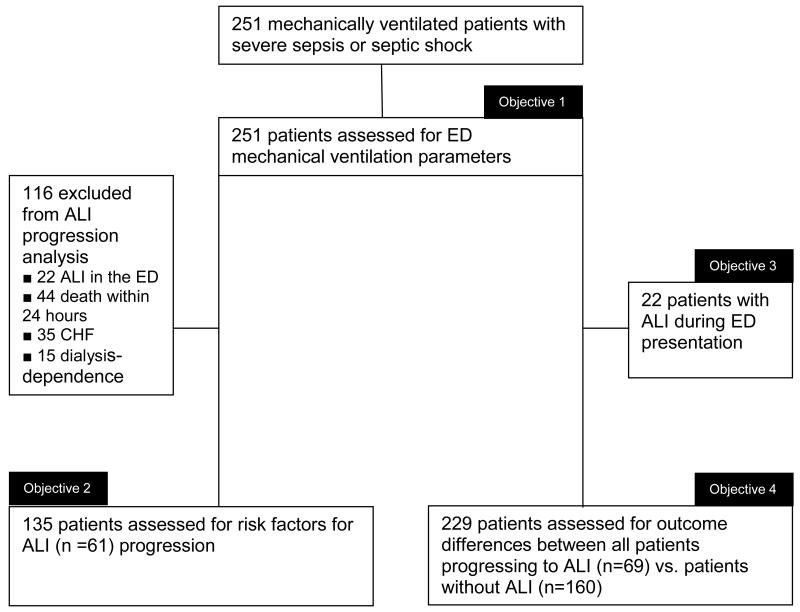
Methods: This was a retrospective, observational cohort study of mechanically ventilated patients with severe sepsis and septic shock (June 2005 to May 2010), presenting to an academic ED with an annual census of >95,000 patients. All patients in the study (n = 251) were analyzed for characterization of mechanical ventilation use in the ED. The primary outcome variable of interest was the incidence of ALI progression after intensive care unit (ICU) admission from the ED and risk factors present in the ED associated with this outcome. Secondary analyses included ALI present in the ED and clinical outcomes comparing all patients progressing to ALI versus no ALI. To assess predictors of progression to ALI, significant variables in univariable analyses at a p ≤ 0.10 level were candidates for inclusion in a bidirectional, stepwise, multivariable logistic regression analysis.
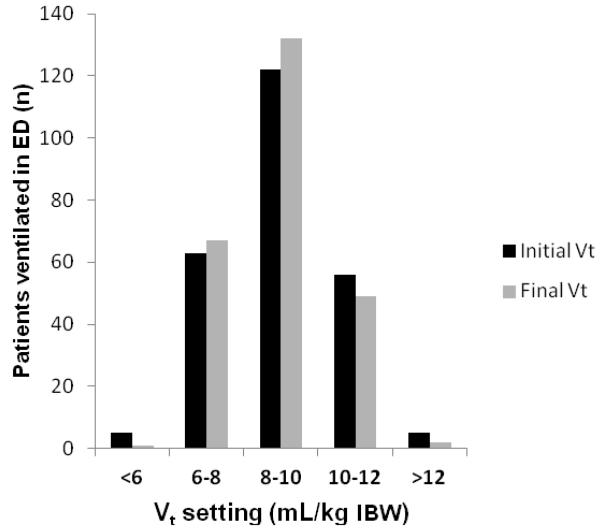
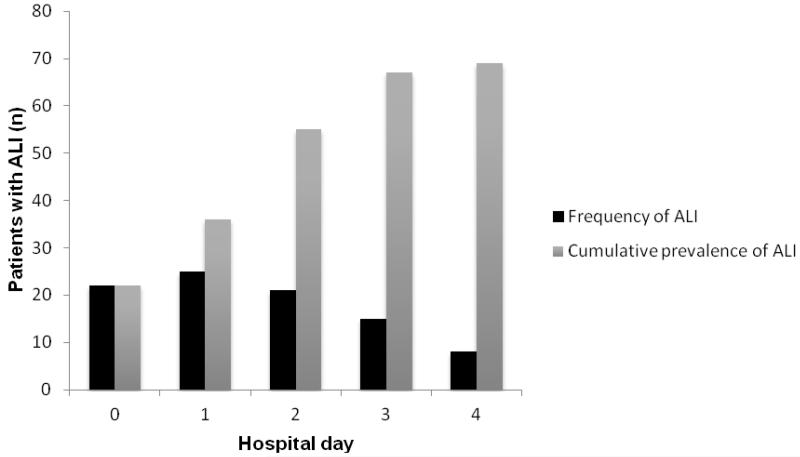
Results: Lung-protective ventilation was used in 68 patients (27.1%) and did not differ based on ALI status. Delivered tidal volume was highly variable, with a median tidal volume delivered of 8.8 mL/kg ideal body weight (IBW; interquartile range [IQR] = 7.8 to 10.0) and a range of 5.2 to 14.6 mL/kg IBW. Sixty-nine patients (27.5%) in the entire cohort progressed to ALI after admission to the hospital, with a mean (±SD) onset of 2.1 (±1) days. Multivariable logistic regression analysis demonstrated that a higher body mass index (BMI), higher Sequential Organ Failure Assessment (SOFA) score, and ED vasopressor use were associated with progression to ALI. There was no association between ED ventilator settings and progression to ALI. Compared to patients who did not progress to ALI, patients progressing to ALI after admission from the ED had an increase in mechanical ventilator duration, vasopressor dependence, and hospital length of stay (LOS).
Conclusions: Lung-protective ventilation is uncommon in the ED, regardless of ALI status. Given the frequency of ALI in the ED, the progression shortly after ICU admission, and the clinical consequences of this syndrome, the effect of ED-based interventions aimed at reducing the sequelae of ALI should be investigated further.
© 2013 by the Society for Academic Emergency Medicine.
Figures
Comment in
-
Mechanical ventilation in the emergency department: a call to action in a resource-constrained era.Acad Emerg Med. 2013 Jul;20(7):746-8. doi: 10.1111/acem.12156. Epub 2013 Jun 12. Acad Emerg Med. 2013. PMID: 23758415 No abstract available.
References
-
- Sagarin MJ, Barton ED, Chng YM, Walls RM. Airway management by US and Canadian emergency medicine residents: a multicenter analysis of more than 6,000 endotracheal intubation attempts. Ann Emerg Med. 2005;46:328–36. - PubMed
-
- Carson SS, Cox CE, Holmes GM, Howard A, Carey TS. The changing epidemiology of mechanical ventilation: a population-based study. J Inten Care Med. 2006;21:173–82. - PubMed
-
- Needham DM, Bronskill SE, Calinawan JR, Sibbald WJ, Pronovost PJ, Laupacis A. Projected incidence of mechanical ventilation in Ontario to 2026: preparing for the aging baby boomers. Crit Care Med. 2005;33:574–9. - PubMed
-
- Fromm RE, Gibbs LR, McCallum WB, et al. Critical care in the emergency department: a time-based study. Crit Care Med. 1993;21:970–6. - PubMed
-
- McCaig LF, Nawar EW. National hospital ambulatory medical care survey: 2004 emergency department summary. Adv Data. 2006;18(340):1–34. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
