

Use and associated risks of concomitant aspirin therapy with oral anticoagulation in patients with atrial fibrillation: insights from the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF) Registry
- PMID: 23861512
- PMCID: PMC3908483
- DOI: 10.1161/CIRCULATIONAHA.113.002927
Use and associated risks of concomitant aspirin therapy with oral anticoagulation in patients with atrial fibrillation: insights from the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF) Registry
Abstract
Background: The role of concomitant aspirin (ASA) therapy in patients with atrial fibrillation (AF) receiving oral anticoagulation (OAC) is unclear. We assessed concomitant ASA use and its association with clinical outcomes among AF patients treated with OAC.
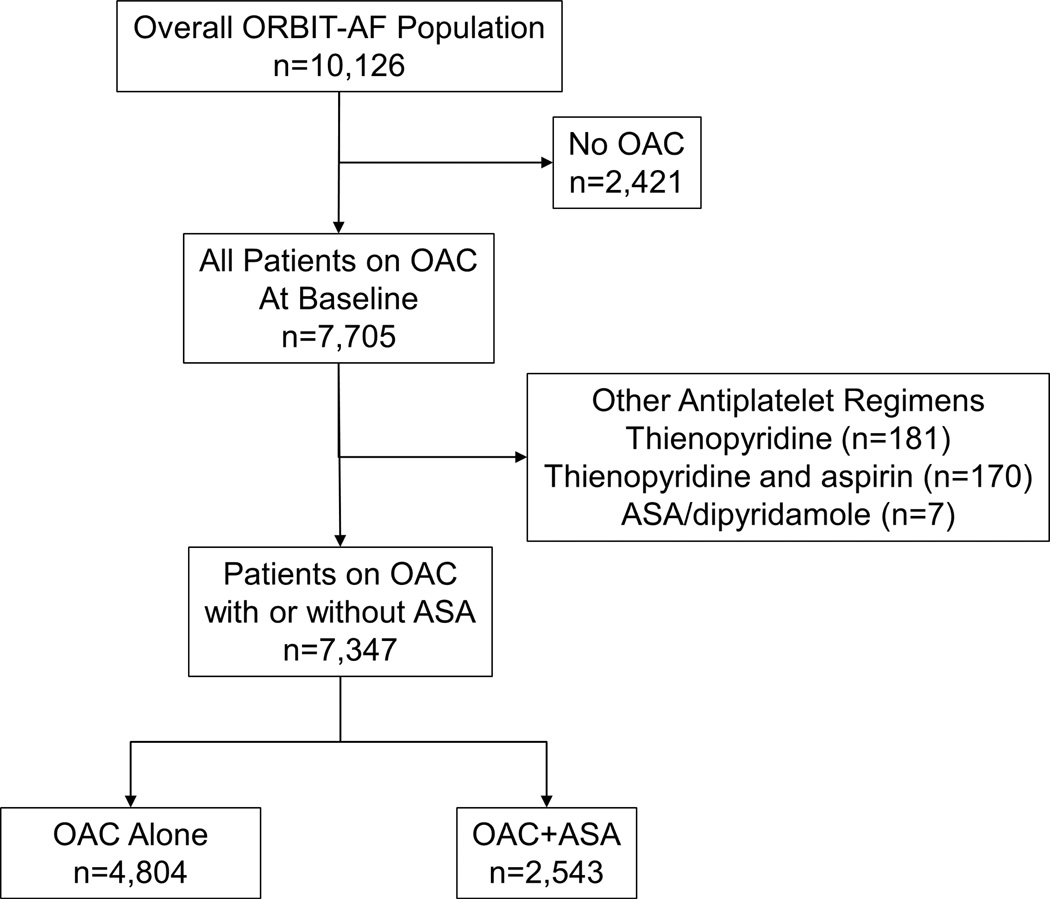
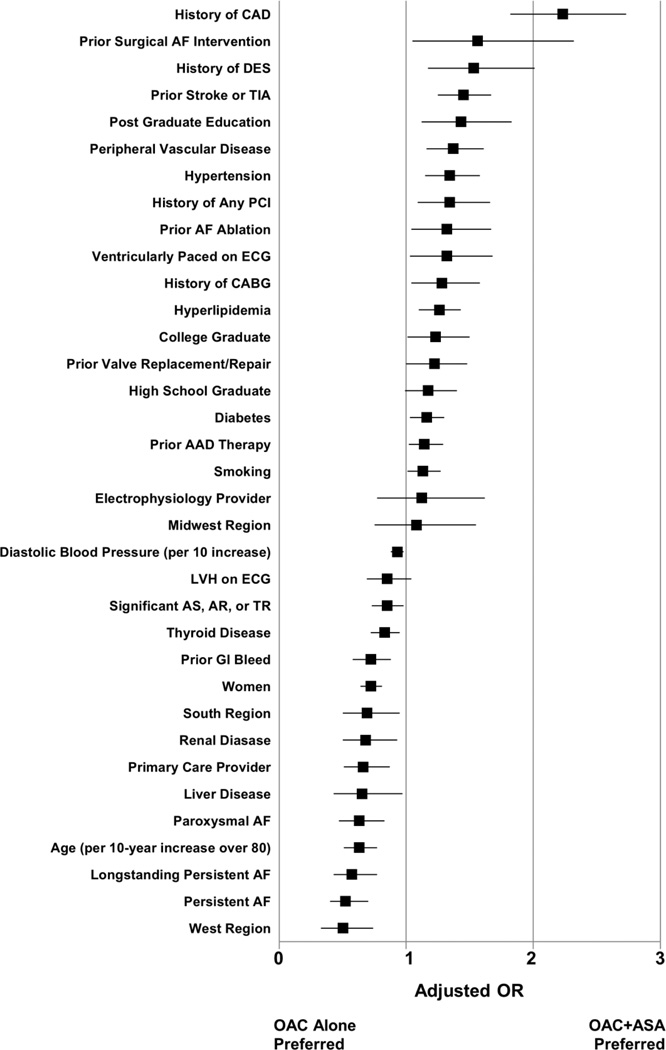
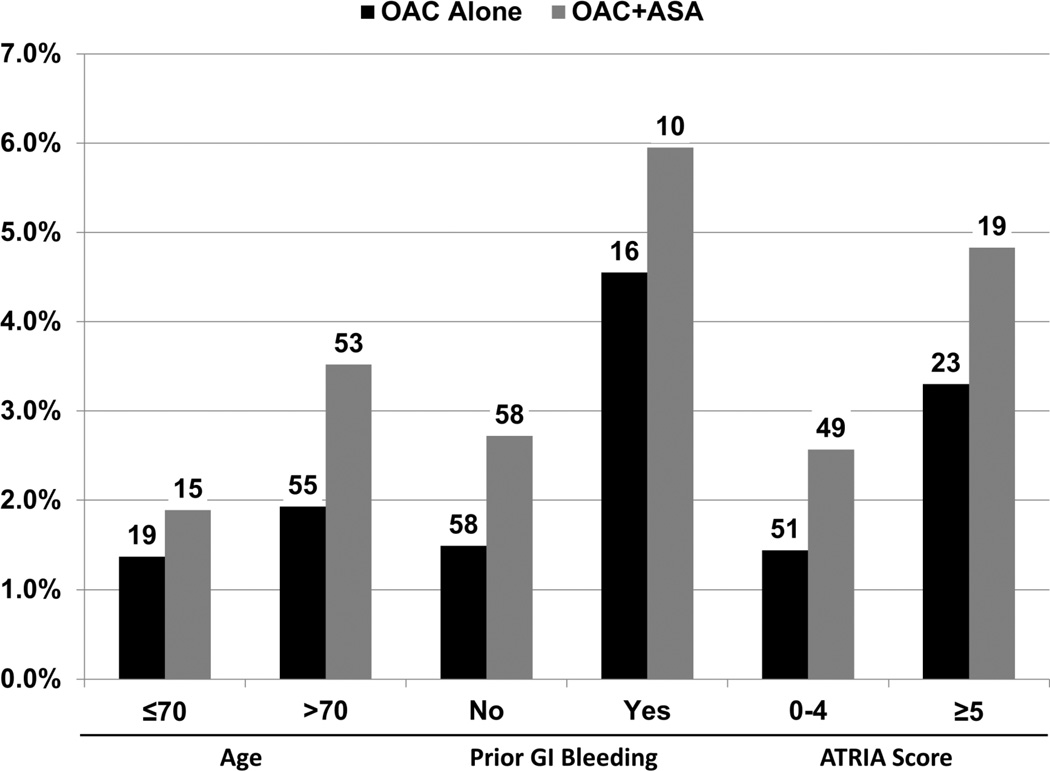
Methods and results: The Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF) registry enrolled 10 126 AF patients from 176 US practices from June 2010 through August 2011. The study population was limited to those on OAC (n=7347). Hierarchical multivariable logistic regression models were used to assess factors associated with concomitant ASA therapy. Primary outcomes were 6-month bleeding, hospitalization, ischemic events, and mortality. Overall, 35% of AF patients (n=2543) on OAC also received ASA (OAC+ASA). Patients receiving OAC+ASA were more likely to be male (66% versus 53%; P<0.0001) and had more comorbid illness than those on OAC alone. More than one third of patients (39%) receiving OAC+ASA did not have a history of atherosclerotic disease, yet 17% had elevated Anticoagulation and Risk Factors in Atrial Fibrillation (ATRIA) bleeding risk scores (≥5). Major bleeding (adjusted hazard ratio, 1.53; 95% confidence interval, 1.20-1.96) and bleeding hospitalizations (adjusted hazard ratio, 1.52; 95% confidence interval, 1.17-1.97) were significantly higher in those on OAC+ASA compared with those on OAC alone. Rates of ischemic events were low.
Conclusions: Patients with AF receiving OAC are often treated with concomitant ASA, even when they do not have cardiovascular disease. Use of OAC+ASA was associated with significantly increased risk for bleeding, emphasizing the need to carefully determine if and when the benefits of concomitant ASA outweigh the risks in AF patients already on OAC.
Clinical trial registration: URL: http://www.clinicaltrials.gov. UNIQUE IDENTIFIER: NCT01165710.
Keywords: anticoagulants; aspirin; atrial fibrillation; hemorrhage; outcome assessment (health care).
Conflict of interest statement
Figures
Comment in
-
Antithrombotic therapy for patients with atrial fibrillation and atherothrombotic vascular disease: striking the right balance between efficacy and safety.Circulation. 2013 Aug 13;128(7):684-6. doi: 10.1161/CIRCULATIONAHA.113.004564. Epub 2013 Jul 16. Circulation. 2013. PMID: 23861513 No abstract available.
References
-
- Lloyd-Jones DM. Lifetime risk for development of atrial fibrillation: The framingham heart study. Circulation. 2004;110:1042–1046. - PubMed
-
- Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: The framingham study. Stroke. 1991;22:983–988. - PubMed
-
- Lopes RD, Pieper KS, Horton JR, Al-Khatib SM, Newby LK, Mehta RH, Van de Werf F, Armstrong PW, Mahaffey KW, Harrington RA, Ohman EM, White HD, Wallentin L, Granger CB. Short- and long-term outcomes following atrial fibrillation in patients with acute coronary syndromes with or without st-segment elevation. Heart. 2008;94:867–873. - PubMed
-
- Camm AJ, Kirchhof P, Lip GY, Schotten U, Savelieva I, Ernst S, Van Gelder IC, Al-Attar N, Hindricks G, Prendergast B, Heidbuchel H, Alfieri O, Angelini A, Atar D, Colonna P, De Caterina R, De Sutter J, Goette A, Gorenek B, Heldal M, Hohloser SH, Kolh P, Le Heuzey JY, Ponikowski P, Rutten FH. Guidelines for the management of atrial fibrillation: The task force for the management of atrial fibrillation of the european society of cardiology (esc) Euro Heart J. 2010;31:2369–2429. - PubMed
-
- Fuster V, Ryden LE, Cannom DS, Crijns HJ, Curtis AB, Ellenbogen KA, Halperin JL, Kay GN, Le Huezey JY, Lowe JE, Olsson SB, Prystowsky EN, Tamargo JL, Wann LS, Smith SC, Jr, Priori SG, Estes NA, 3rd, Ezekowitz MD, Jackman WM, January CT, Page RL, Slotwiner DJ, Stevenson WG, Tracy CM, Jacobs AK, Anderson JL, Albert N, Buller CE, Creager MA, Ettinger SM, Guyton RA, Hochman JS, Kushner FG, Ohman EM, Tarkington LG, Yancy CW. 2011 accf/aha/hrs focused updates incorporated into the acc/aha/esc 2006 guidelines for the management of patients with atrial fibrillation: A report of the american college of cardiology foundation/american heart association task force on practice guidelines. Circulation. 2011;123:e269–e367. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
