

Balancing evidence and uncertainty when considering rubella vaccine introduction
- PMID: 23861777
- PMCID: PMC3702572
- DOI: 10.1371/journal.pone.0067639
Balancing evidence and uncertainty when considering rubella vaccine introduction
Abstract
Background: Despite a safe and effective vaccine, rubella vaccination programs with inadequate coverage can raise the average age of rubella infection; thereby increasing rubella cases among pregnant women and the resulting congenital rubella syndrome (CRS) in their newborns. The vaccination coverage necessary to reduce CRS depends on the birthrate in a country and the reproductive number, R0, a measure of how efficiently a disease transmits. While the birthrate within a country can be known with some accuracy, R0 varies between settings and can be difficult to measure. Here we aim to provide guidance on the safe introduction of rubella vaccine into countries in the face of substantial uncertainty in R0.
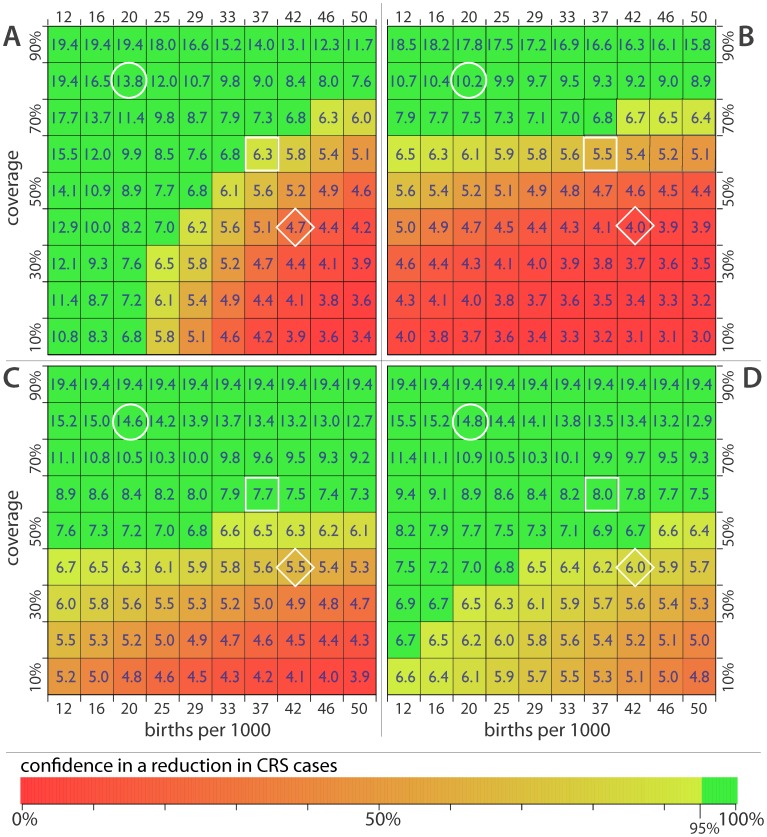
Methods: We estimated the distribution of R0 in African countries based on the age distribution of rubella infection using Bayesian hierarchical models. We developed an age specific model of rubella transmission to predict the level of R0 that would result in an increase in CRS burden for specific birth rates and coverage levels. Combining these results, we summarize the safety of introducing rubella vaccine across demographic and coverage contexts.
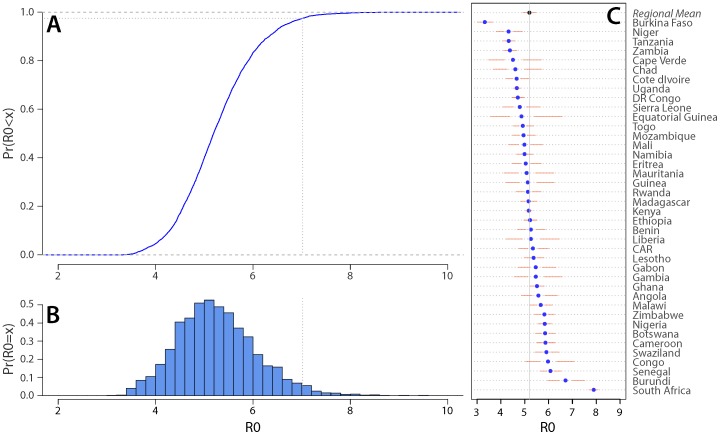
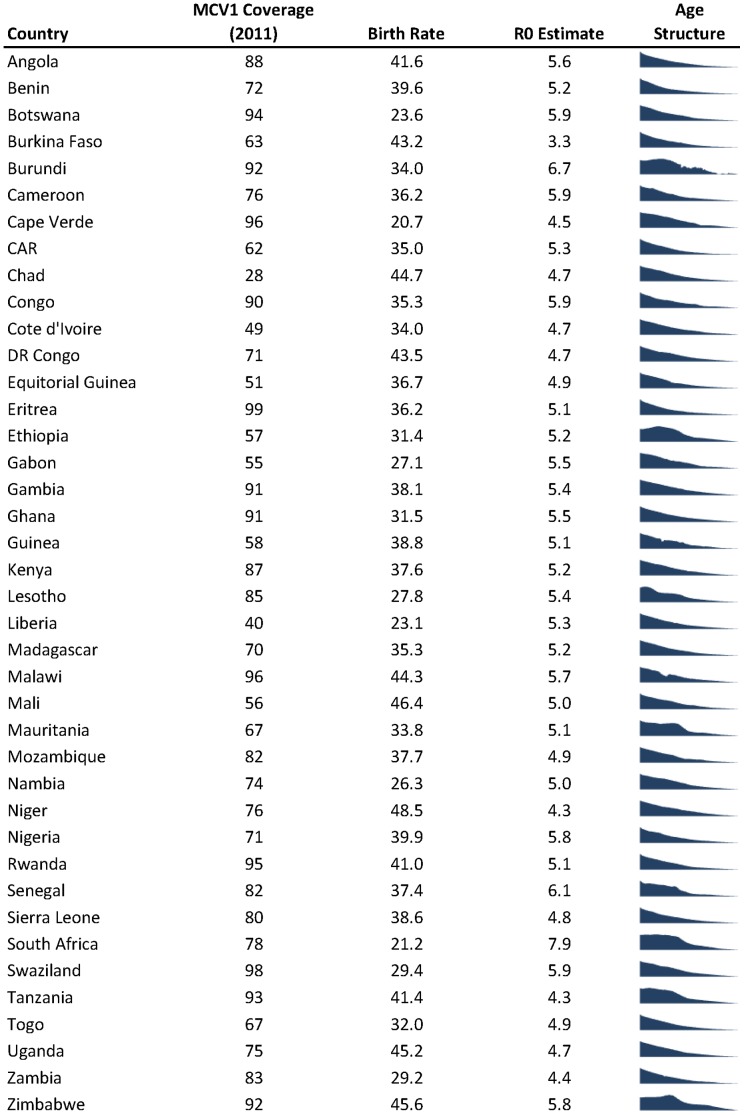
Findings: The median R0 of rubella in the African region is 5.2, with 90% of countries expected to have an R0 between 4.0 and 6.7. Overall, we predict that countries maintaining routine vaccination coverage of 80% or higher are can be confident in seeing a reduction in CRS over a 30 year time horizon.
Conclusions: Under realistic assumptions about human contact, our results suggest that even in low birth rate settings high vaccine coverage must be maintained to avoid an increase in CRS. These results lend further support to the WHO recommendation that countries reach 80% coverage for measles vaccine before introducing rubella vaccination, and highlight the importance of maintaining high levels of vaccination coverage once the vaccine is introduced.
Conflict of interest statement
Figures
Similar articles
-
Impact of birth rate, seasonality and transmission rate on minimum levels of coverage needed for rubella vaccination.Epidemiol Infect. 2012 Dec;140(12):2290-301. doi: 10.1017/S0950268812000131. Epub 2012 Feb 16. Epidemiol Infect. 2012. PMID: 22335852 Free PMC article.
-
Informing rubella vaccination strategies in East Java, Indonesia through transmission modelling.Vaccine. 2016 Nov 4;34(46):5636-5642. doi: 10.1016/j.vaccine.2016.09.010. Epub 2016 Sep 23. Vaccine. 2016. PMID: 27670077
-
Rubella vaccination in India: identifying broad consequences of vaccine introduction and key knowledge gaps.Epidemiol Infect. 2018 Jan;146(1):65-77. doi: 10.1017/S0950268817002527. Epub 2017 Dec 4. Epidemiol Infect. 2018. PMID: 29198212 Free PMC article.
-
Congenital rubella syndrome: a matter of concern.Rev Panam Salud Publica. 2015 Mar;37(3):179-86. Rev Panam Salud Publica. 2015. PMID: 25988255 Review.
-
Targeting rubella for elimination.Indian J Public Health. 2012 Oct-Dec;56(4):269-72. doi: 10.4103/0019-557X.106413. Indian J Public Health. 2012. PMID: 23354136 Review.
Cited by
-
Phylogeography of rubella virus in Asia: Vaccination and demography shape synchronous outbreaks.Epidemics. 2019 Sep;28:100346. doi: 10.1016/j.epidem.2019.100346. Epub 2019 May 28. Epidemics. 2019. PMID: 31201039 Free PMC article.
-
Rubella sero-prevalence among children in Kilimanjaro region: a community based study prior to the introduction of rubella vaccine in Tanzania.Ital J Pediatr. 2017 Jul 21;43(1):63. doi: 10.1186/s13052-017-0379-3. Ital J Pediatr. 2017. PMID: 28732540 Free PMC article.
-
Introduction of rubella-containing-vaccine to Madagascar: implications for roll-out and local elimination.J R Soc Interface. 2016 Apr;13(117):20151101. doi: 10.1098/rsif.2015.1101. J R Soc Interface. 2016. PMID: 27122178 Free PMC article.
-
Development and dissemination of infectious disease dynamic transmission models during the COVID-19 pandemic: what can we learn from other pathogens and how can we move forward?Lancet Digit Health. 2021 Jan;3(1):e41-e50. doi: 10.1016/S2589-7500(20)30268-5. Epub 2020 Dec 7. Lancet Digit Health. 2021. PMID: 33735068 Free PMC article. Review.
-
The geography of measles vaccination in the African Great Lakes region.Nat Commun. 2017 May 25;8:15585. doi: 10.1038/ncomms15585. Nat Commun. 2017. PMID: 28541287 Free PMC article.
References
-
- Jimenez G, Avila-Aguero ML, Morice A, Gutierrez H, Soriano A, et al. (2007) Estimating the burden of Congenital Rubella Syndrome in Costa Rica, 1996–2001. The Pediatric Infectious Disease Journal 26: 382–386. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
