

Decreasing fertility rate correlates with the chronological increase and geographical variation in incidence of Kawasaki disease in Japan
- PMID: 23861836
- PMCID: PMC3704585
- DOI: 10.1371/journal.pone.0067934
Decreasing fertility rate correlates with the chronological increase and geographical variation in incidence of Kawasaki disease in Japan
Abstract
Background: Kawasaki disease (KD) is a common cause of acquired paediatric heart disease in developed countries. KD was first identified in the 1960s in Japan, and has been steadily increasing since it was first reported. The aetiology of KD has not been defined, but is assumed to be infection-related. The present study sought to identify the factor(s) that mediate the geographical variation and chronological increase of KD in Japan.
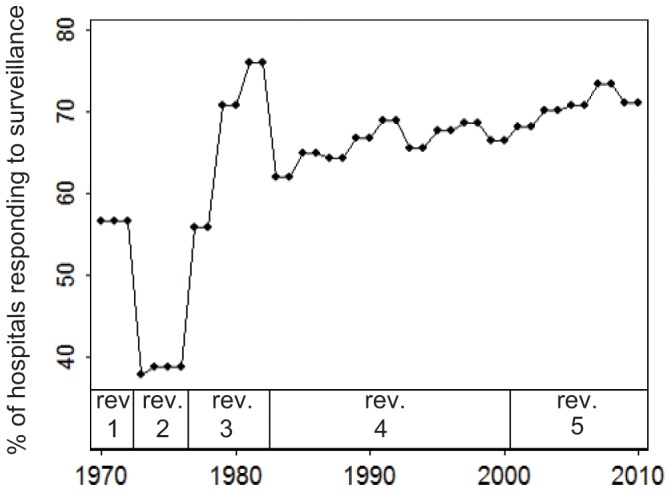
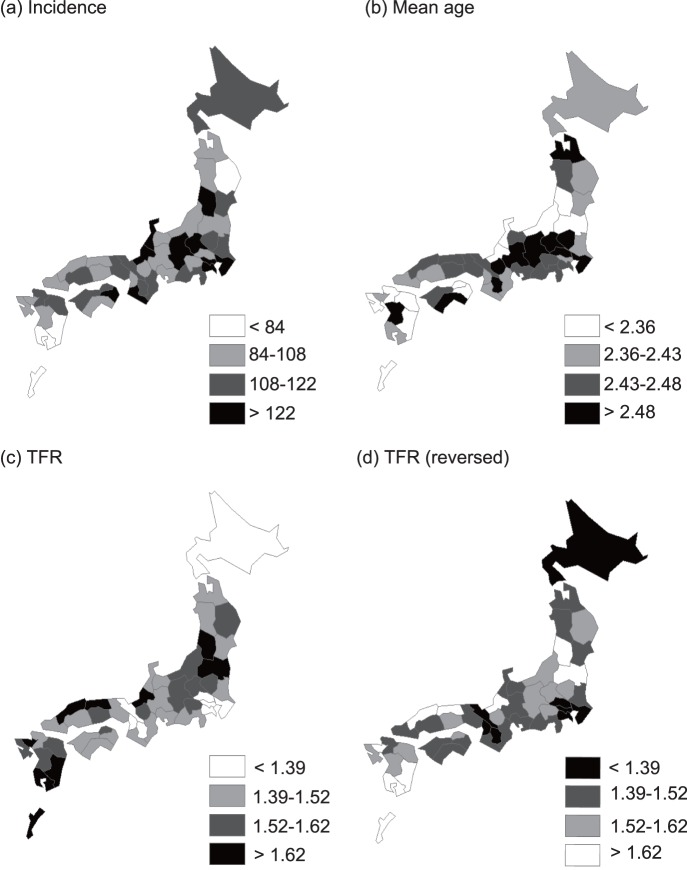
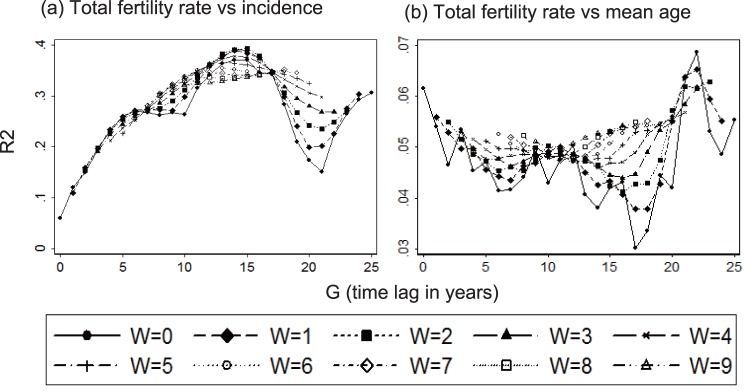
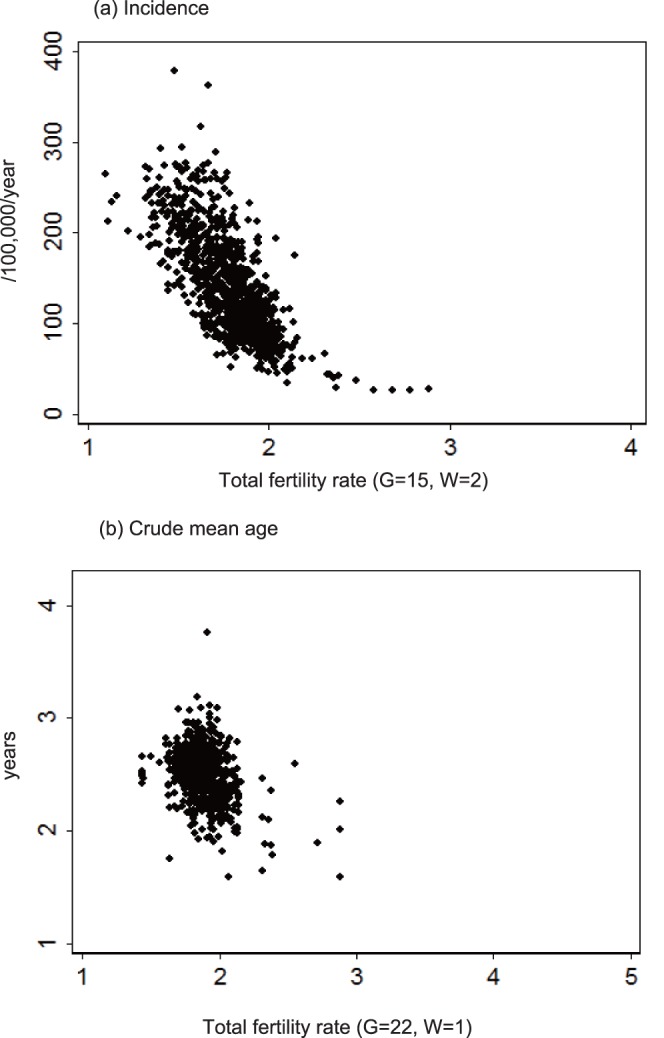
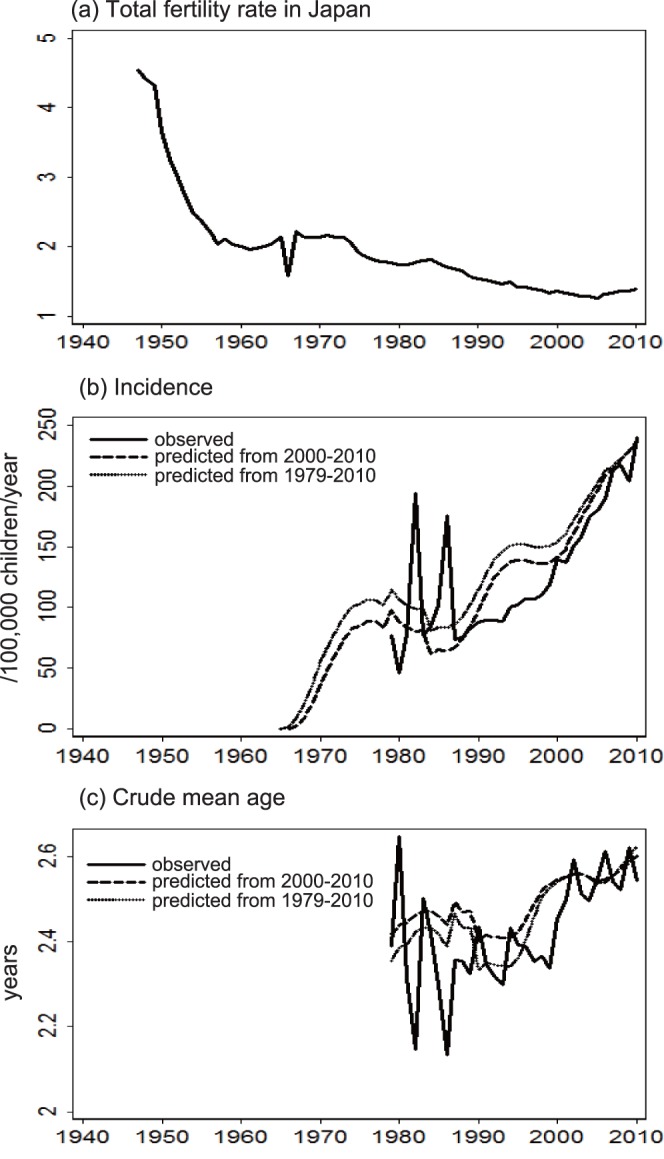
Methods and findings: Based upon data reported between 1979 and 2010 from all 47 prefectures in Japan, the incidence and mean patient age at the onset of KD were estimated. Using spatial and time-series analyses, incidence and mean age were regressed against climatic/socioeconomic variables. Both incidence and mean age of KD were inversely correlated with the total fertility rate (TFR; i.e., the number of children that would be born to one woman). The extrapolation of a time-series regressive model suggested that KD emerged in the 1960s because of a dramatic decrease in TFR in the 1940s through the 1950s.
Conclusions: Mean patient age is an inverse surrogate for the hazard of contracting the aetiologic agent. Therefore, the observed negative correlation between mean patient age and TFR suggests that a higher TFR is associated with KD transmission. This relationship may be because a higher TFR facilitates sibling-to-sibling transmission. Additionally, the observed inverse correlation between incidence and TFR implies a paradoxical "negative" correlation between the incidence and the hazard of contracting the aetiologic agent. It was hypothesized that a decreasing TFR resulted in a reduced hazard of contracting the agent for KD, thereby increasing KD incidence.
Conflict of interest statement
Figures
References
-
- Kawasaki T (1967) Acute febrile mucocutaneous syndrome with lymphoid involvement with specific desquamation of the fingers and toes in children (in Japanese). Arerugi 16: 178–222. - PubMed
-
- Kato H, Koike S, Yamamoto M, Ito Y, Yano E (1975) Coronary aneurysms in infants and young children with acute febrile mucocutaneous lymph node syndrome. J Pediatr 86: 892–898. - PubMed
-
- Furusho K, Kamiya T, Nakano H, Kiyosawa N, Shinomiya K, et al. (1984) High-dose intravenous gammaglobulin for Kawasaki disease. Lancet 324: 1055–1058. - PubMed
-
- Newburger JW, Takahashi M, Burns JC, Beiser AS, Chung KJ, et al. (1986) The treatment of Kawasaki syndrome with intravenous gamma globulin. N Engl J Med 315: 341–347. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
