

When are statins cost-effective in cardiovascular prevention? A systematic review of sponsorship bias and conclusions in economic evaluations of statins
- PMID: 23861972
- PMCID: PMC3704635
- DOI: 10.1371/journal.pone.0069462
When are statins cost-effective in cardiovascular prevention? A systematic review of sponsorship bias and conclusions in economic evaluations of statins
Abstract
Background: We examined sponsorship of published cost-effectiveness analyses of statin use for cardiovascular (CV) prevention, and determined whether the funding source is associated with study conclusions.
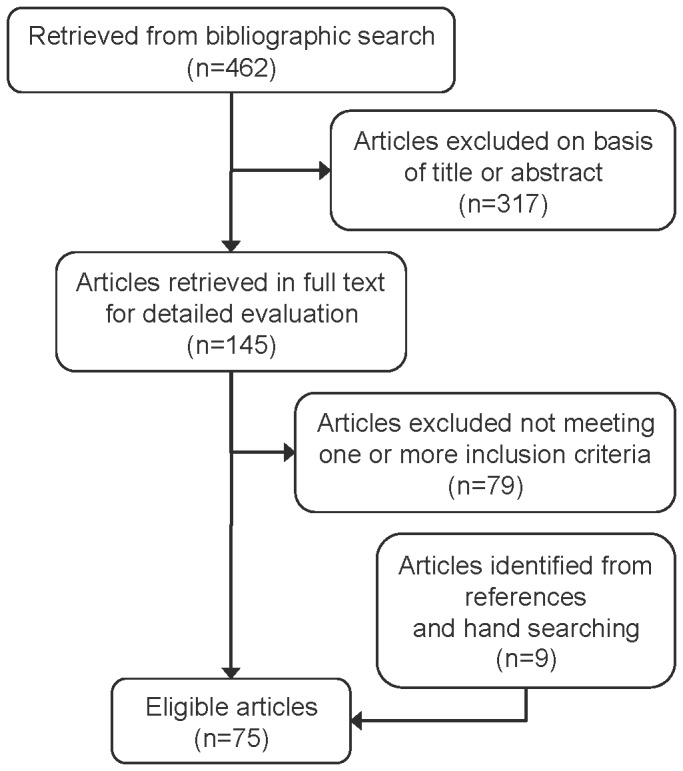
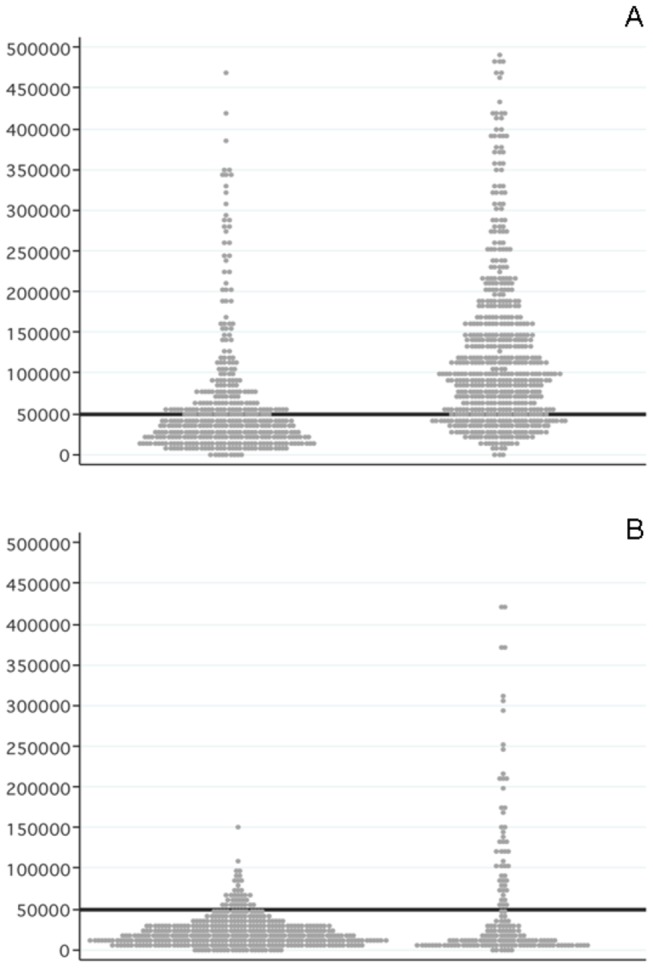
Methods and findings: We searched PubMed/MEDLINE (up to June 2011) to identify cost-effectiveness analyses of statin use for CV prevention reporting outcomes as incremental costs per quality-adjusted life years (QALY) and/or life years gained (LYG). We examined relationships between the funding source and the study conclusions by means of tests of differences between proportions. Seventy-five studies were included. Forty-eight studies (64.0%) were industry-sponsored. Fifty-two (69.3%) articles compared statins versus non-active alternatives. Secondary CV prevention represented 42.7% of articles, followed by primary CV prevention (38.7%) and both (18.7%). Overall, industry-sponsored studies were much less likely to report unfavourable or neutral conclusions (0% versus 37.1%; p<0.001). For primary CV prevention, the proportion with unfavourable or neutral conclusions was 0% for industry-sponsored studies versus 57.9% for non-sponsored studies (p<0.001). Conversely, no statistically significant differences were identified for studies evaluating secondary CV prevention (0% versus 12.5%; p=0.222). Incremental costs per QALY/LYG estimates reported in industry-sponsored studies were generally more likely to fall below a hypothetical willingness-to-pay threshold of US $50,000.
Conclusions: Our systematic analysis suggests that pharmaceutical industry sponsored economic evaluations of statins have generally favored the cost-effectiveness profile of their products particularly in primary CV prevention.
Conflict of interest statement
Figures
References
-
- Weinstein MC, Stason WB (1977) Foundations of cost-effectiveness analysis for health and medical practices. N Engl J Med 296: 716-721. doi:10.1056/NEJM197703312961304. PubMed: 402576. - DOI - PubMed
-
- Hutton J, McGrath C, Frybourg JM, Tremblay M, Bramley-Harker E et al. (2006) Framework for describing and classifying decision-making systems using technology assessment to determine the reimbursement of health technologies (fourth hurdle systems). Int J Technol Assess Health Care. 22: 10-18. PubMed: 16673675. - PubMed
-
- Greenberg D, Rosen AB, Wacht O, Palmer J, Neumann PJ (2010) A bibliometric review of cost-effectiveness analyses in the economic and medical literature: 1976-2006. Med Decis Mak. 30: 320-327. doi:10.1177/0272989X09360066. - DOI - PubMed
-
- Bell CM, Urbach DR, Ray JG, Bayoumi A, Rosen AB et al. (2006) Bias in published cost effectiveness studies: systematic review. BMJ. 332: 699-703. doi:10.1136/bmj.38737.607558.80. PubMed: 16495332. - DOI - PMC - PubMed
-
- Miners AH, Garau M, Fidan D, Fischer AJ (2005) Comparing estimates of cost effectiveness submitted to the National Institute for Clinical Excellence (NICE) by different organisations: retrospective study. BMJ. 330: 65. doi:10.1136/bmj.38285.482350.82. PubMed: 15601681. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
