

Imaging lymphatic system in breast cancer patients with magnetic resonance lymphangiography
- PMID: 23861979
- PMCID: PMC3702586
- DOI: 10.1371/journal.pone.0069701
Imaging lymphatic system in breast cancer patients with magnetic resonance lymphangiography
Abstract
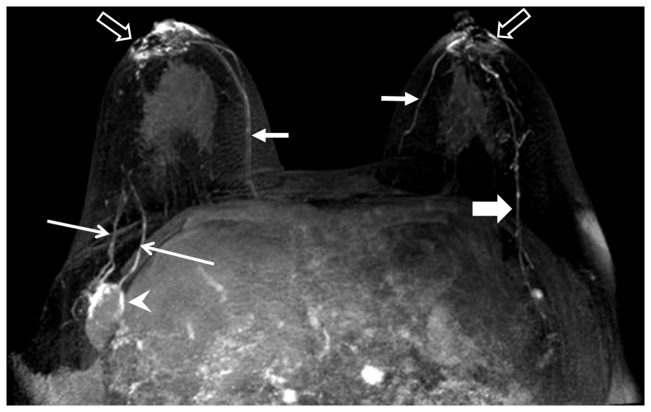
Objective: To investigate the feasibility of gadolinium (Gd) contrast-enhanced magnetic resonance lymphangiography (MRL) in breast cancer patients within a typical clinical setting, and to establish a Gd-MRL protocol and identify potential MRL biomarkers for differentiating metastatic from non-metastatic lymph nodes.
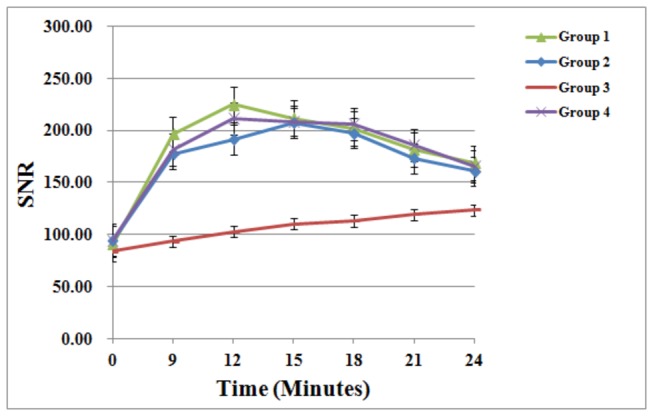
Materials and methods: 32 patients with unilateral breast cancer were enrolled and divided into 4 groups of 8 patients. Groups I, II, and III received 1.0, 0.5, and 0.3 ml of intradermal contrast; group IV received two 0.5 ml doses of intradermal contrast. MRL images were acquired on a 3.0 T system and evaluated independently by two radiologists for the number and size of enhancing lymph nodes, lymph node contrast uptake kinetics, lymph vessel size, and contrast enhancement patterns within lymph nodes.
Results: Group III patients had a statistically significant decrease in the total number of enhancing axillary lymph nodes and lymphatic vessels compared to all other groups. While group IV patients had a statistically significant faster time to reach the maximum peak enhancement over group I and II (by 3 minutes), there was no other statistically significant difference between imaging results between groups I, II, and IV. 27 out of 128 lymphatic vessels (21%) showed dilatation, and all patients with dilated lymphatic vessels were pathologically proven to have metastases. Using the pattern of enhancement defects as the sole criterion for identifying metastatic lymph nodes during Gd-MRL interpretation, and using histopathology as the gold standard, the sensitivity and specificity were estimated to be 86% and 95%, respectively.
Conclusion: Gd-MRL can adequately depict the lymphatic system, can define sentinel lymph nodes, and has the potential to differentiate between metastatic and non-metastatic lymph nodes in breast cancer patients.
Conflict of interest statement
Figures

References
-
- Jemal A, Bray F, Center MM, Ferlay J, Ward E et al. (2011) Global cancer statistics. CA Cancer J Clin 61: 69-90. doi:10.3322/caac.20107. PubMed: 21296855. - DOI - PubMed
-
- Overgaard M, Nielsen HM, Overgaard J (2007) Is the benefit of postmastectomy irradiation limited to patients with four or more positive nodes, as recommended in international consensus reports? A subgroup analysis of the DBCG 82 b&c randomized trials. Radiother Oncol 82: 247-253. doi:10.1016/j.radonc.2007.02.001. PubMed: 17306393. - DOI - PubMed
-
- Veronesi U, Paganelli G, Viale G, Galimberti V, Luini A et al. (1999) Sentinel lymph node biopsy and axillary dissection in breast cancer: results in a large series. J Natl Cancer Inst 91: 368-373. doi:10.1093/jnci/91.4.368. PubMed: 10050871. - DOI - PubMed
-
- Tanis PJ, Nieweg OE, Valdés Olmos RA, Kroon BB (2001) Anatomy and physiology of lymphatic drainage of the breast from the perspective of sentinel node biopsy. J Am Coll Surg 192: 399-409. doi:10.1016/S1072-7515(00)00776-6. PubMed: 11245383. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
