

Atypical sleep in ventilated patients: empirical electroencephalography findings and the path toward revised ICU sleep scoring criteria
- PMID: 23863228
- PMCID: PMC3875326
- DOI: 10.1097/CCM.0b013e31828a3f75
Atypical sleep in ventilated patients: empirical electroencephalography findings and the path toward revised ICU sleep scoring criteria
Abstract
Objectives: Standard sleep scoring criteria may be unreliable when applied to critically ill patients. We sought to quantify typical and atypical polysomnographic findings in critically ill patients and to begin development and reliability testing of methodology to characterize the atypical polysomnographic tracings that confound standard sleep scoring criteria.
Design: Prospective convenience sample.
Setting: Two academic, tertiary care medical centers.
Patients: Thirty-seven critically ill, mechanically ventilated, medical ICU patients.
Interventions: None.
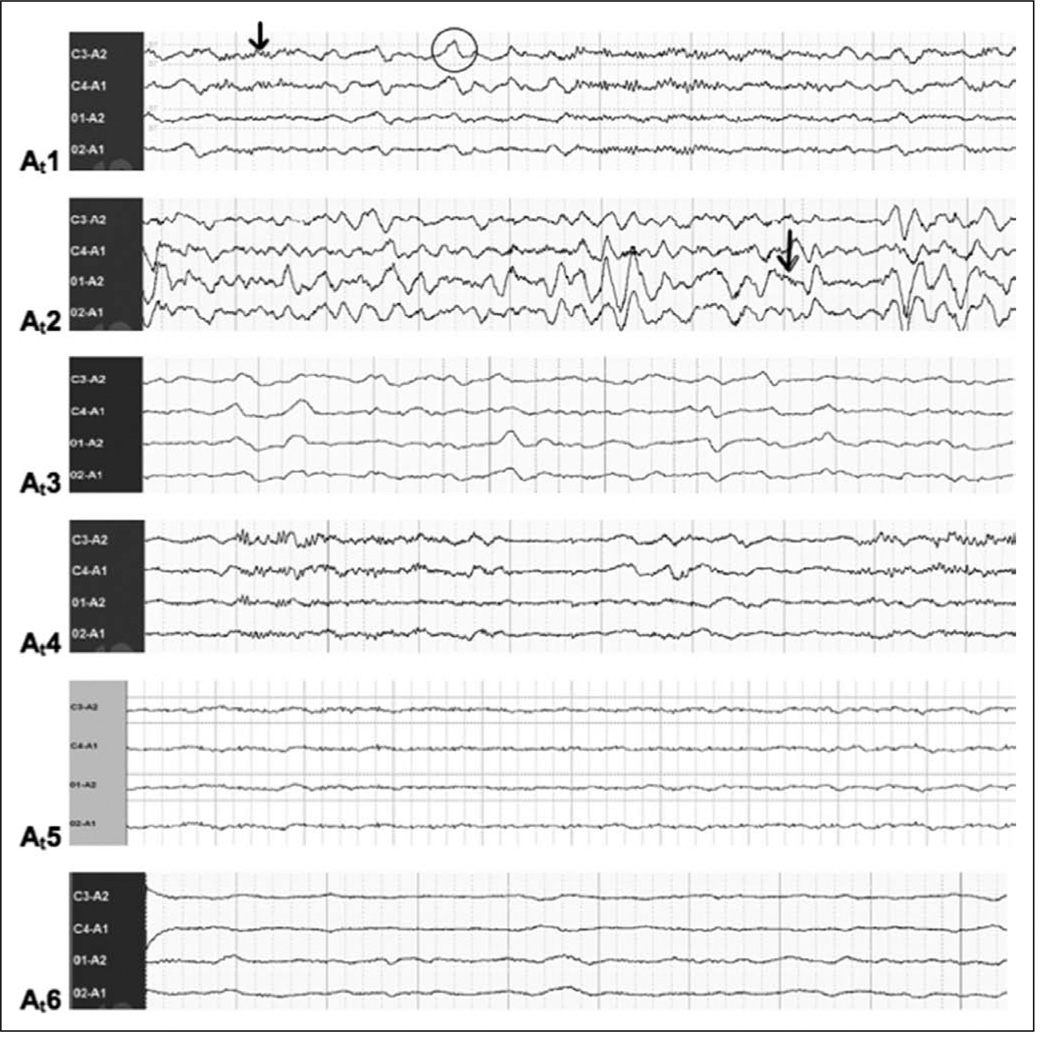
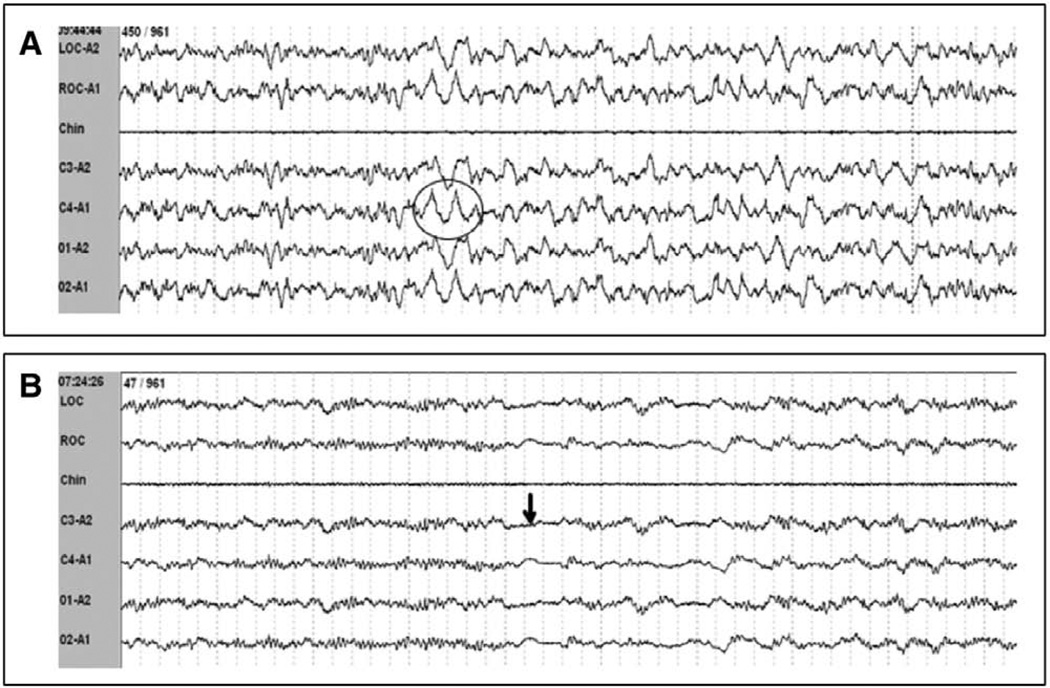
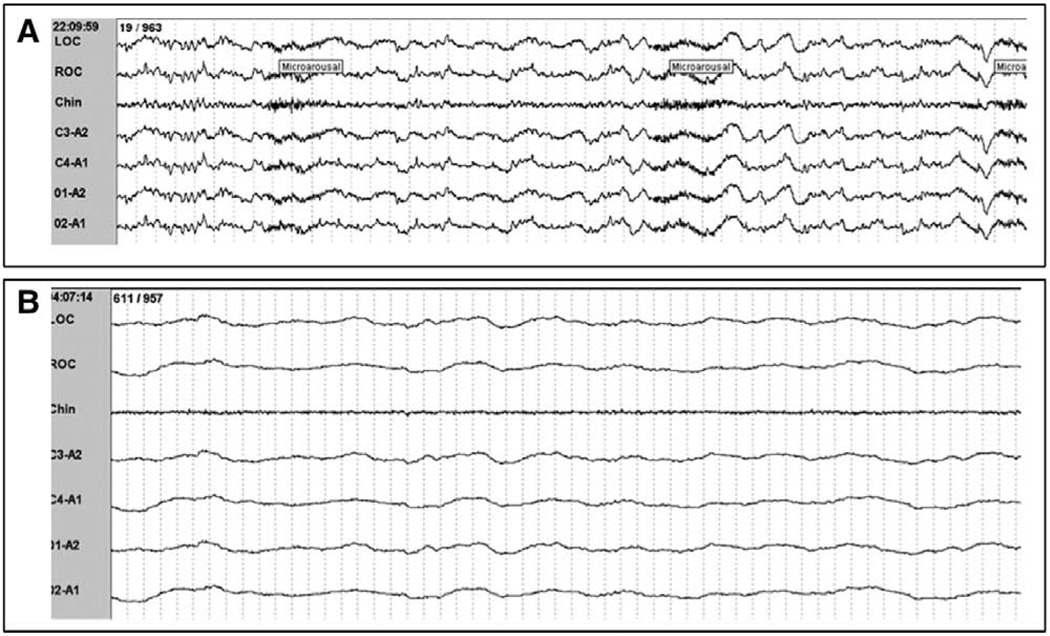
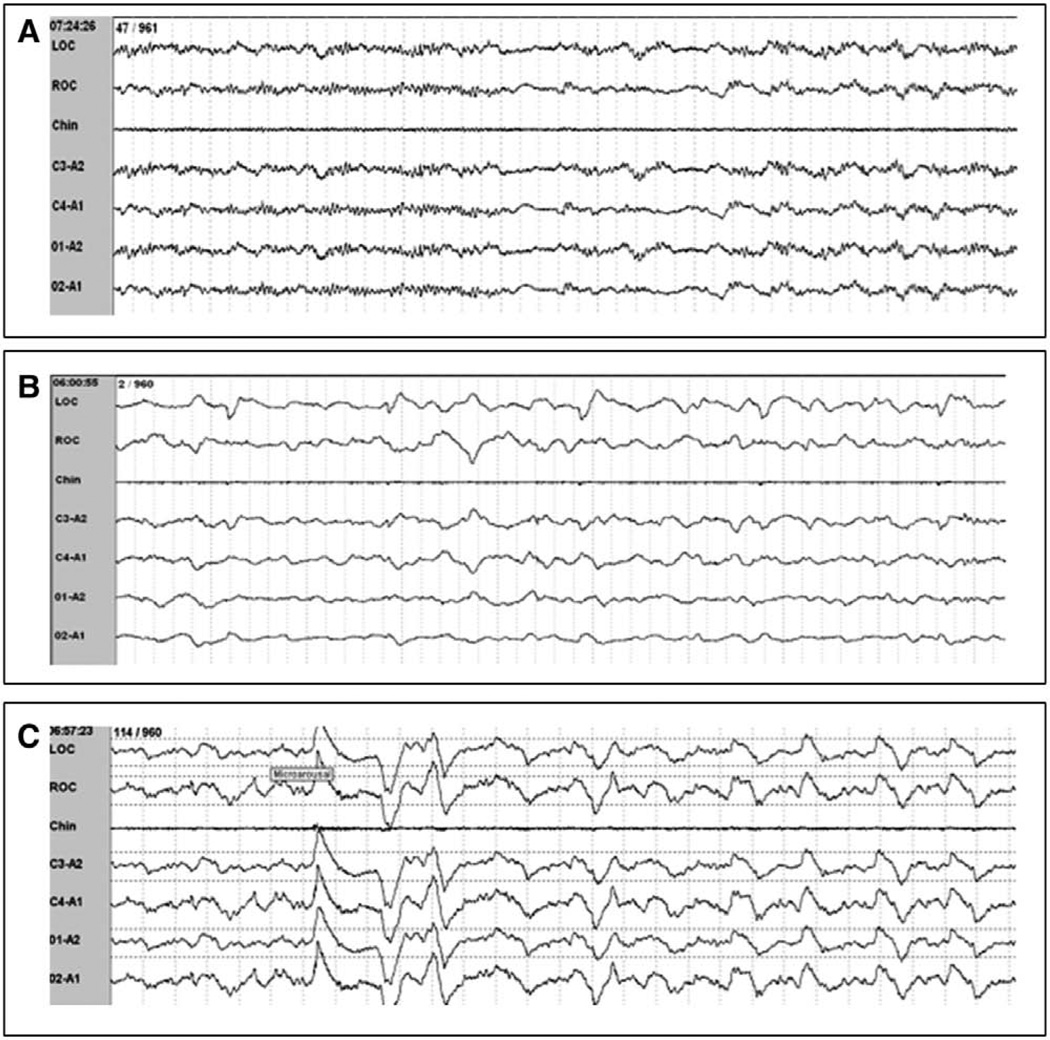
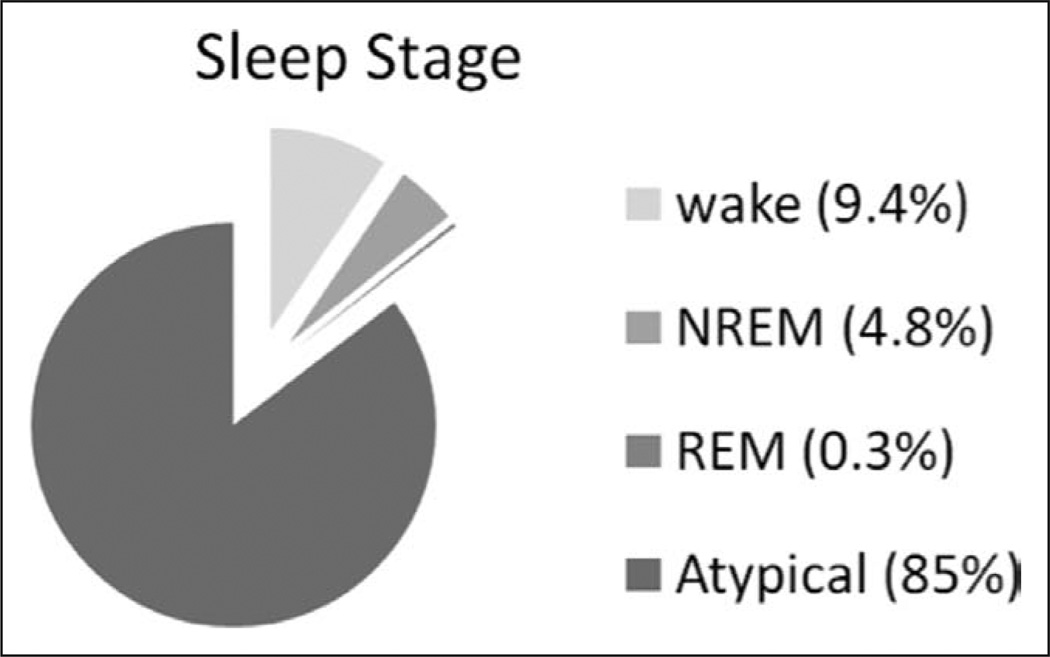
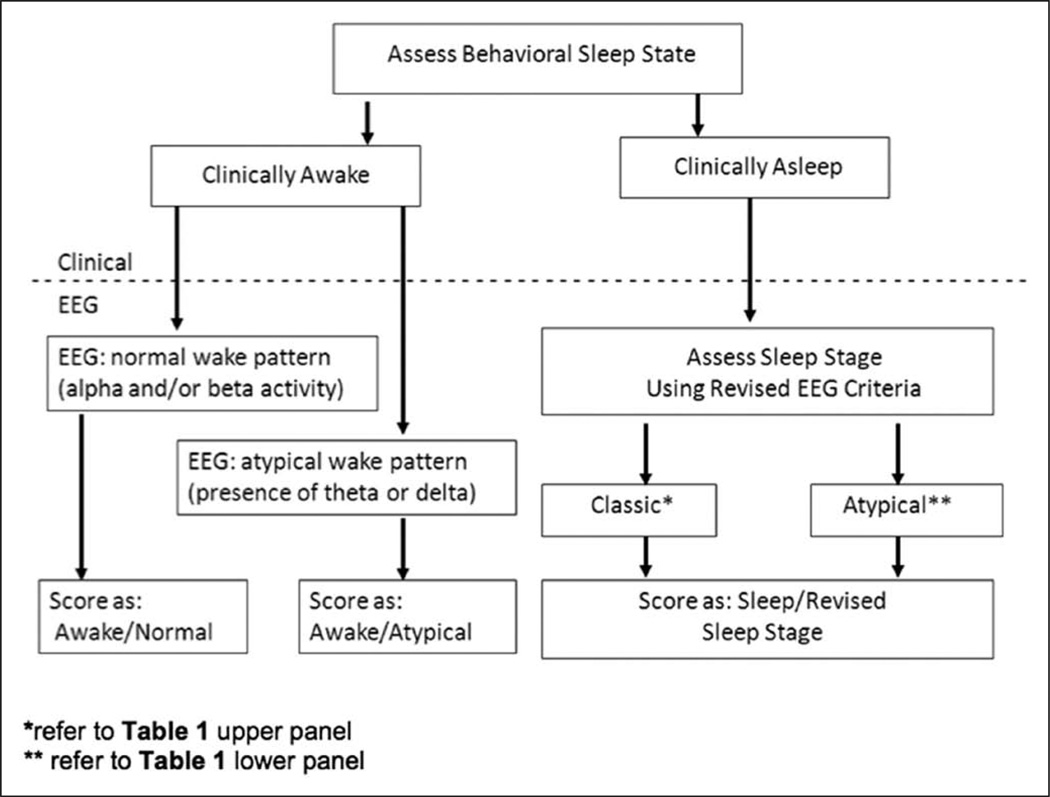
Measurements and main results: Mechanically ventilated subjects were monitored by continuous polysomnography. After noting frequent atypical polysomnographic findings (i.e., lack of stage N2 markers, the presence of polymorphic delta, burst suppression, or isoelectric electroencephalography), attempts to use standard sleep scoring criteria alone were abandoned. Atypical polysomnographic findings were characterized and used to develop a modified scoring system. Polysomnographic data were scored manually via this revised scoring scheme. Of 37 medical ICU patients enrolled, 36 experienced atypical sleep, which accounted for 85% of all recorded data, with 5.1% normal sleep and 9.4% wake. Coupling observed patient arousal levels with polysomnographic characteristics revealed that standard polysomnographic staging criteria did not reliably determine the presence or absence of sleep. Rapid eye movement occurred in only five patients (14%). The revised scoring system incorporating frequently seen atypical characteristics yielded very high interrater reliability (weighted κ = 0.80; bootstrapped 95% CI, [0.48, 0.89]).
Conclusions: Analysis of polysomnographic data revealed profound deficiencies in standard scoring criteria due to a predominance of atypical polysomnographic findings in ventilated patients. The revised scoring scheme proved reliable in sleep staging and may serve as a building block in future work.
Conflict of interest statement
Dr. Thompson has disclosed that she does not have any potential conflicts of interest.
Figures
Comment in
-
Sleep in ICU: atypical sleep or atypical electroencephalography?Crit Care Med. 2014 Apr;42(4):e312-3. doi: 10.1097/CCM.0000000000000158. Crit Care Med. 2014. PMID: 24633122 No abstract available.
-
The authors reply.Crit Care Med. 2014 Apr;42(4):e313-4. doi: 10.1097/CCM.0000000000000207. Crit Care Med. 2014. PMID: 24633123 No abstract available.
References
-
- Cooper AB, Thornley KS, Young GB, et al. Sleep in critically ill patients requiring mechanical ventilation. Chest. 2000;117:809–818. - PubMed
-
- Freedman NS, Gazendam J, Levan L, et al. Abnormal sleep/wake cycles and the effect of environmental noise on sleep disruption in the intensive care unit. Am J Respir Crit Care Med. 2001;163:451–457. - PubMed
-
- Helton MC, Gordon SH, Nunnery SL. The correlation between sleep deprivation and the intensive care unit syndrome. Heart Lung. 1980;9:464–468. - PubMed
-
- Trompeo AC, Vidi Y, Locane MD, et al. Sleep disturbances in the critically ill patients: Role of delirium and sedative agents. Minerva Anestesiol. 2011;77:604–612. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
