

Differences in medical therapy goals for children with severe traumatic brain injury-an international study
- PMID: 23863819
- PMCID: PMC4455880
- DOI: 10.1097/PCC.0b013e3182975e2f
Differences in medical therapy goals for children with severe traumatic brain injury-an international study
Abstract
Objectives: To describe the differences in goals for their usual practice for various medical therapies from a number of international centers for children with severe traumatic brain injury.
Design: A survey of the goals from representatives of the international centers.
Setting: Thirty-two pediatric traumatic brain injury centers in the United States, United Kingdom, France, and Spain.
Patients: None.
Interventions: None.
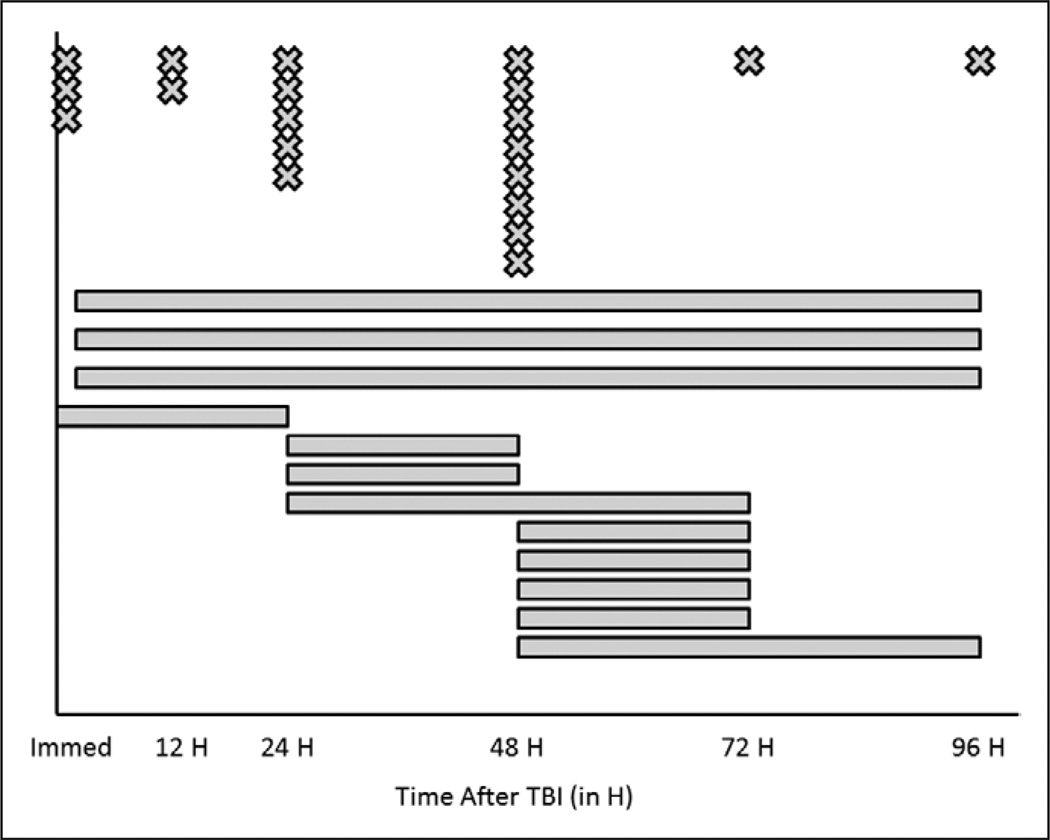
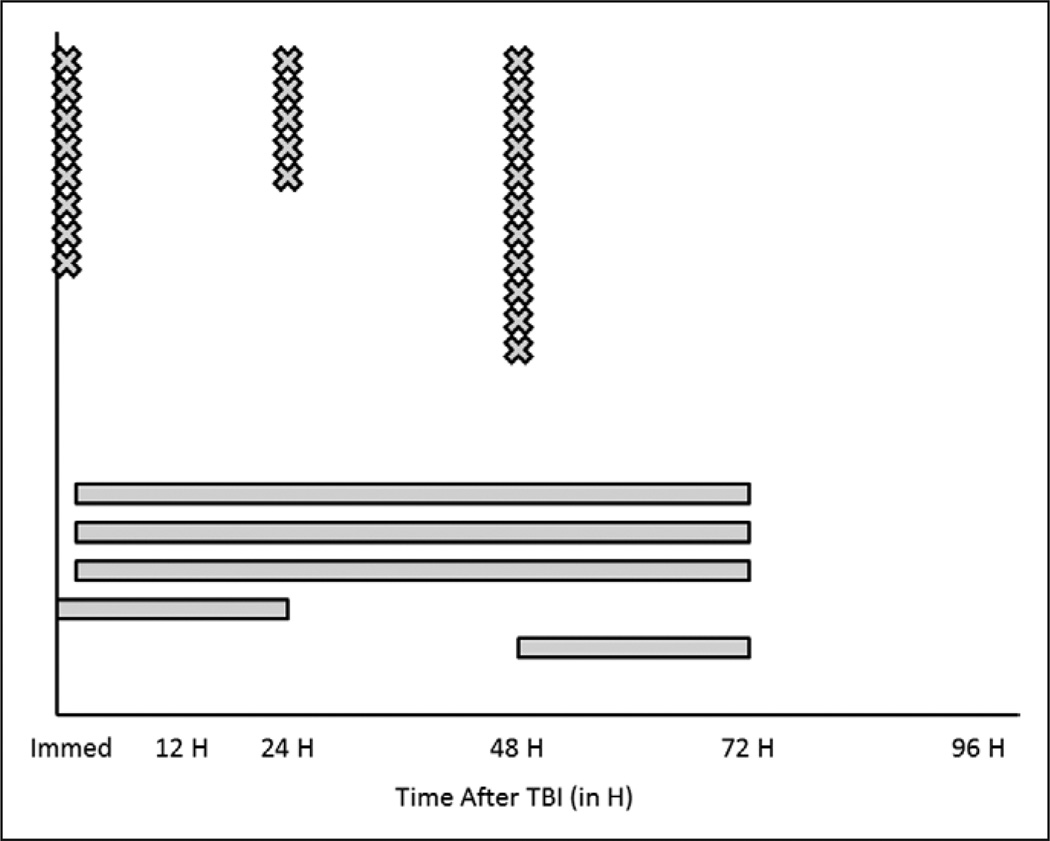
Measurements and main results: A survey instrument was developed that required free-form responses from the centers regarding their usual practice goals for topics of intracranial hypertension therapies, hypoxia/ischemia prevention and detection, and metabolic support. Cerebrospinal fluid diversion strategies varied both across centers and within centers, with roughly equal proportion of centers adopting a strategy of continuous cerebrospinal fluid diversion and a strategy of no cerebrospinal fluid diversion. Use of mannitol and hypertonic saline for hyperosmolar therapies was widespread among centers (90.1% and 96.9%, respectively). Of centers using hypertonic saline, 3% saline preparations were the most common but many other concentrations were in common use. Routine hyperventilation was not reported as a standard goal and 31.3% of centers currently use PbO(2) monitoring for cerebral hypoxia. The time to start nutritional support and glucose administration varied widely, with nutritional support beginning before 96 hours and glucose administration being started earlier in most centers.
Conclusions: There were marked differences in medical goals for children with severe traumatic brain injury across our international consortium, and these differences seemed to be greatest in areas with the weakest evidence in the literature. Future studies that determine the superiority of the various medical therapies outlined within our survey would be a significant advance for the pediatric neurotrauma field and may lead to new standards of care and improved study designs for clinical trials.
Conflict of interest statement
The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Faul MD, Xu L, Wald MM, et al. Traumatic Brain Injury in the United States: Emergency Department Visits, Hospitalizations and Death 2002–2006. Atlanta GA: Centers for Disease Control and Prevention, National Center for Injury Prevention; 2010.
-
- Stocchetti N, Conte V, Ghisoni L, et al. Traumatic brain injury in pediatric patients. Minerva Anestesiol. 2010;76:1052–1059. - PubMed
-
- Tude Melo JR, Di Rocco F, Blanot S, et al. Mortality in children with severe head trauma: Predictive factors and proposal for a new predictive scale. Neurosurgery. 2010;67:1542–1547. - PubMed
Publication types
MeSH terms
Grants and funding
- U01 CE001630/CE/NCIPC CDC HHS/United States
- NS052478/NS/NINDS NIH HHS/United States
- MH085722/MH/NIMH NIH HHS/United States
- U01 NS081041/NS/NINDS NIH HHS/United States
- MH56612/MH/NIMH NIH HHS/United States
- T32HD040686/HD/NICHD NIH HHS/United States
- R10 MH056612/MH/NIMH NIH HHS/United States
- U44 NS070324/NS/NINDS NIH HHS/United States
- R01 NS069247/NS/NINDS NIH HHS/United States
- F32 HD008003/HD/NICHD NIH HHS/United States
- U01 NS052478/NS/NINDS NIH HHS/United States
- NS070324/NS/NINDS NIH HHS/United States
- R01 NS072308/NS/NINDS NIH HHS/United States
- NS069247/NS/NINDS NIH HHS/United States
- R01 MH056612/MH/NIMH NIH HHS/United States
- HD08003/HD/NICHD NIH HHS/United States
- CAPMC/ CIHR/Canada
- HD0499893/HD/NICHD NIH HHS/United States
- R01 MH085722/MH/NIMH NIH HHS/United States
- NS072308/NS/NINDS NIH HHS/United States
- T32 HD040686/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
