Which patients might benefit from postmastectomy radiotherapy in breast cancer patients with t1-2 tumor and 1-3 axillary lymph nodes metastasis?
- PMID: 23864843
- PMCID: PMC3710959
- DOI: 10.4143/crt.2013.45.2.103
Which patients might benefit from postmastectomy radiotherapy in breast cancer patients with t1-2 tumor and 1-3 axillary lymph nodes metastasis?
Abstract
Purpose: This study compared the clinical outcomes of T1-2N1 breast cancer patients with and without postmastectomy radiotherapy (PMRT). Risk factors for loco-regional recurrence (LRR) were identified in order to define a subgroup of patients who might benefit from PMRT.
Materials and methods: Of 110 T1-2N1 breast cancer patients who underwent mastectomy from January 1994 through December 2009, 32 patients underwent PMRT and 78 patients did not. Treatment outcomes and risk factors for LRR were analyzed.
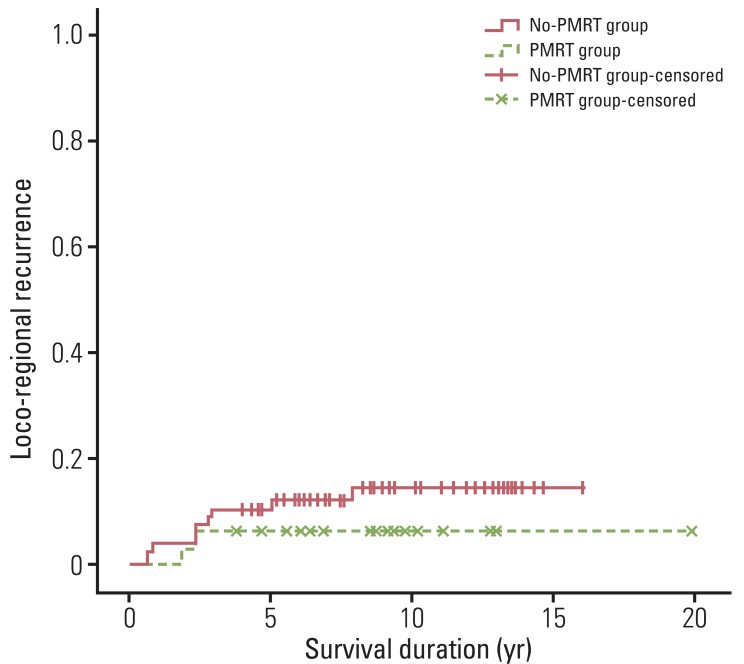
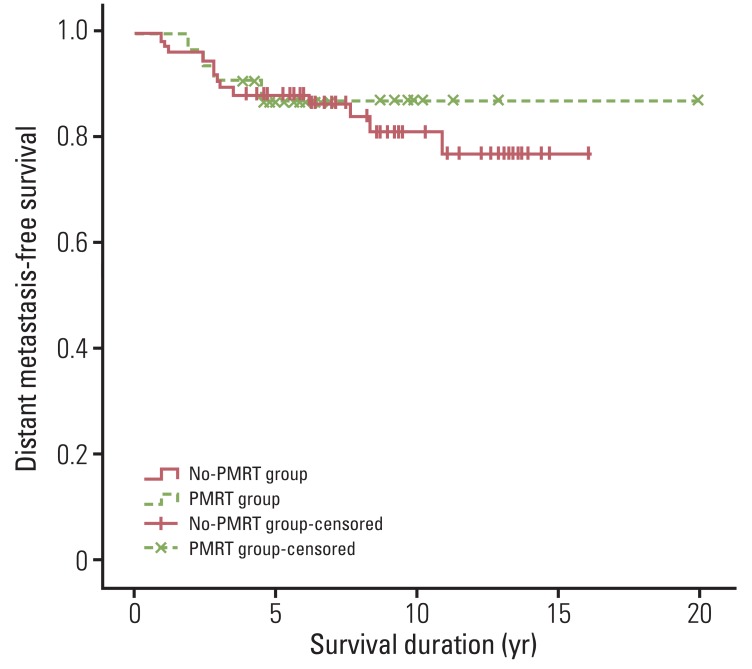
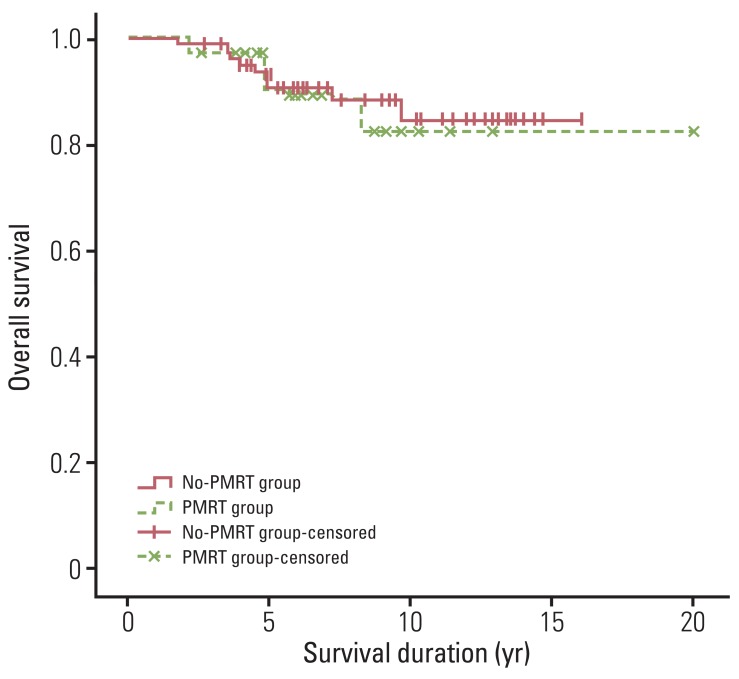
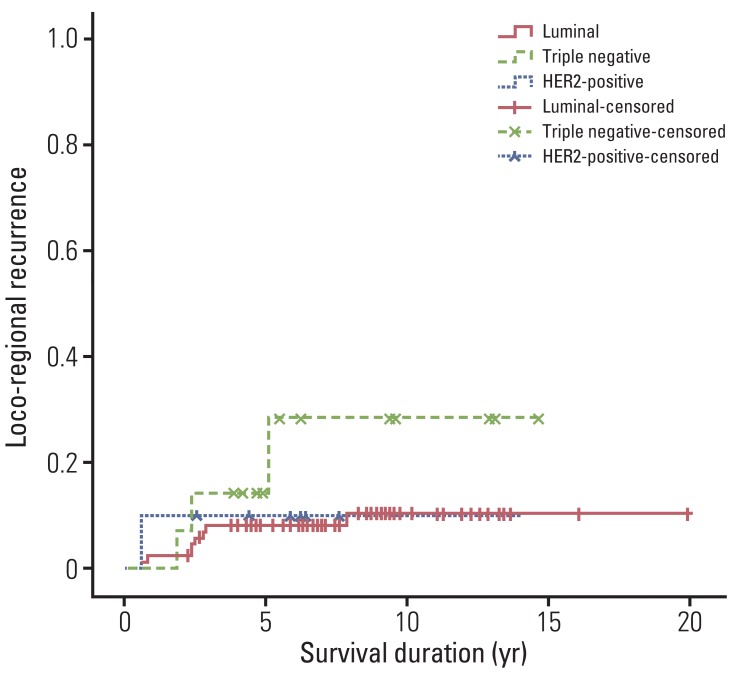
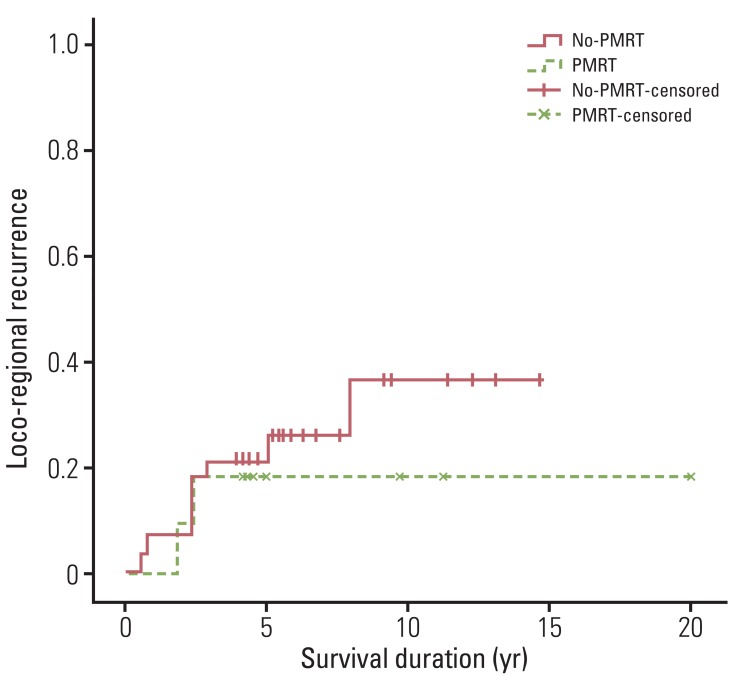
Results: The 5- and 10-year LRR rates were both 6.2% in the PMRT group, and 10.4% and 14.6% in the no-PMRT group (p=0.336). In addition, no significant differences in distant metastasis-free survival (DMFS) or overall survival (OS) were observed between patients receiving and not receiving PMRT. In multivariate analysis, factors associated with higher LRR rates included grade 3 disease, extracapsular extension (ECE), and triple negative subtype. Patients who had one or more risk factors for LRR were defined as a high-risk patient group. In the high-risk group, both 5- and 10-year LRR rates for patients who underwent PMRT was 18.2%, and LRR rates of 21.4% at five years and 36.6% at 10 years were observed for patients who did not undergo PMRT (p=0.069).
Conclusion: PMRT in T1-2N1 breast cancer patients should be considered according to several prognostic factors in addition to T and N stage. Findings of our study indicated that PMRT did not improve LRR, DMFS, or OS in T1-2N1 breast cancer patients. However, in a subgroup of patients with grade 3 disease, ECE, or triple negative subtype, PMRT might be beneficial.
Keywords: Breast neoplasms; Mastectomy; Radiotherapy; Risk factor.
Conflict of interest statement
Conflict of interest relevant to this article was not reported.
Figures
References
-
- Ragaz J, Jackson SM, Le N, Plenderleith IH, Spinelli JJ, Basco VE, et al. Adjuvant radiotherapy and chemotherapy in node-positive premenopausal women with breast cancer. N Engl J Med. 1997;337:956–962. - PubMed
-
- Overgaard M, Hansen PS, Overgaard J, Rose C, Andersson M, Bach F, et al. Postoperative radiotherapy in high-risk premenopausal women with breast cancer who receive adjuvant chemotherapy. Danish Breast Cancer Cooperative Group 82b Trial. N Engl J Med. 1997;337:949–955. - PubMed
-
- Overgaard M, Jensen MB, Overgaard J, Hansen PS, Rose C, Andersson M, et al. Postoperative radiotherapy in high-risk postmenopausal breast-cancer patients given adjuvant tamoxifen: Danish Breast Cancer Cooperative Group DBCG 82c randomised trial. Lancet. 1999;353:1641–1648. - PubMed
-
- Whelan TJ, Julian J, Wright J, Jadad AR, Levine ML. Does locoregional radiation therapy improve survival in breast cancer? A meta-analysis. J Clin Oncol. 2000;18:1220–1229. - PubMed
-
- Recht A, Edge SB, Solin LJ, Robinson DS, Estabrook A, Fine RE, et al. Postmastectomy radiotherapy: clinical practice guidelines of the American Society of Clinical Oncology. J Clin Oncol. 2001;19:1539–1569. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources