

Operation of a brain-computer interface walking simulator for individuals with spinal cord injury
- PMID: 23866985
- PMCID: PMC3723437
- DOI: 10.1186/1743-0003-10-77
Operation of a brain-computer interface walking simulator for individuals with spinal cord injury
Abstract
Background: Spinal cord injury (SCI) can leave the affected individuals with paraparesis or paraplegia, thus rendering them unable to ambulate. Since there are currently no restorative treatments for this population, novel approaches such as brain-controlled prostheses have been sought. Our recent studies show that a brain-computer interface (BCI) can be used to control ambulation within a virtual reality environment (VRE), suggesting that a BCI-controlled lower extremity prosthesis for ambulation may be feasible. However, the operability of our BCI has not yet been tested in a SCI population.
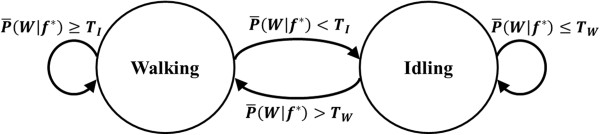
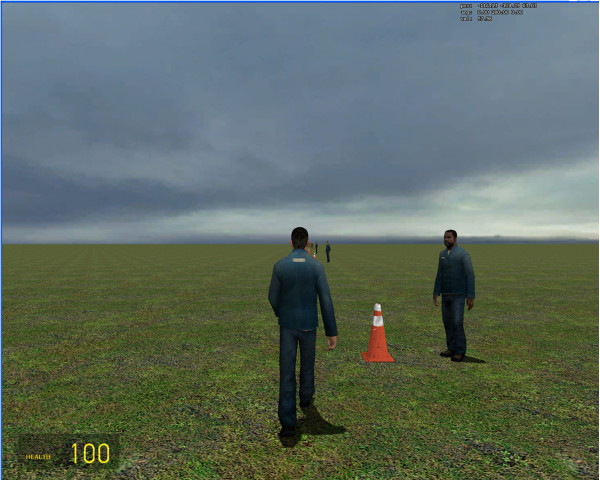
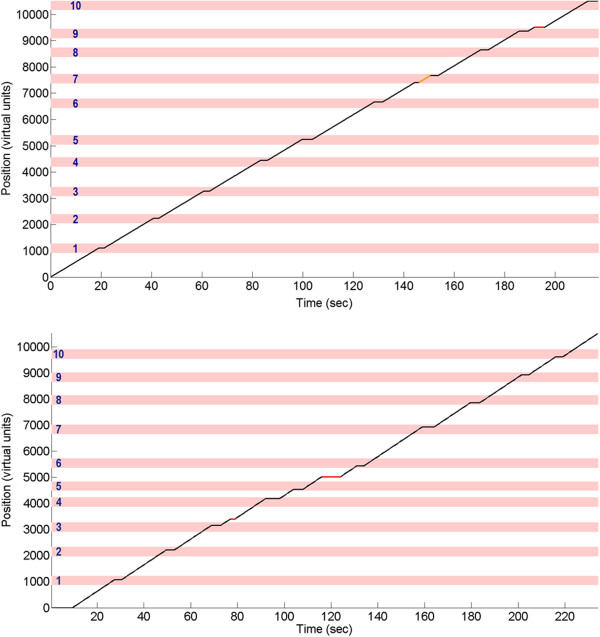
Methods: Five participants with paraplegia or tetraplegia due to SCI underwent a 10-min training session in which they alternated between kinesthetic motor imagery (KMI) of idling and walking while their electroencephalogram (EEG) were recorded. Participants then performed a goal-oriented online task, where they utilized KMI to control the linear ambulation of an avatar while making 10 sequential stops at designated points within the VRE. Multiple online trials were performed in a single day, and this procedure was repeated across 5 experimental days.
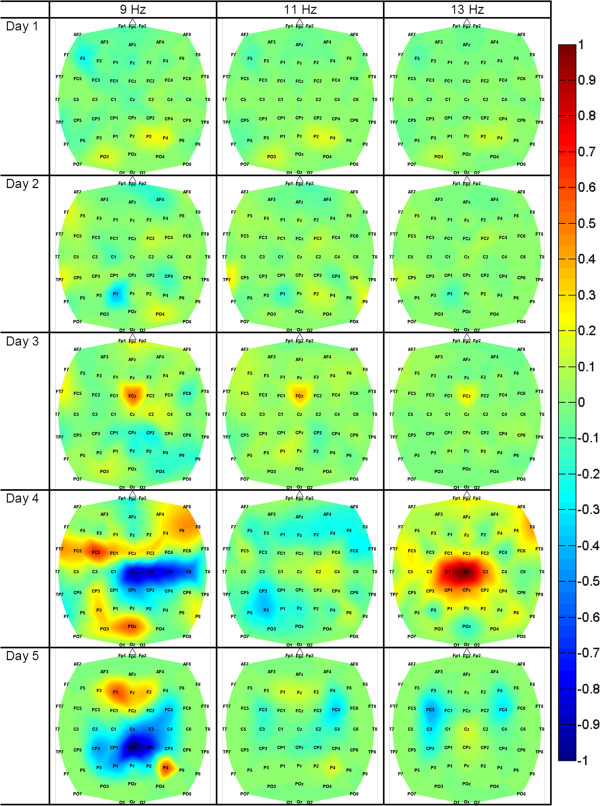
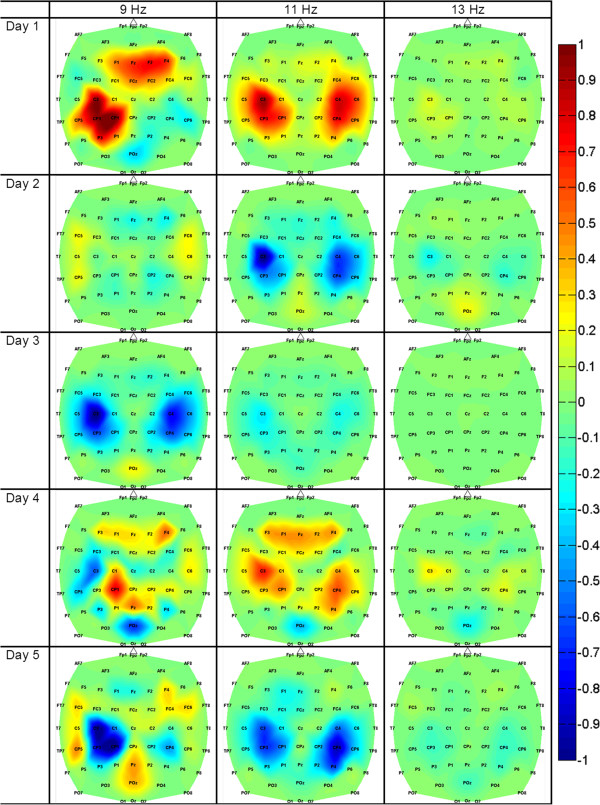
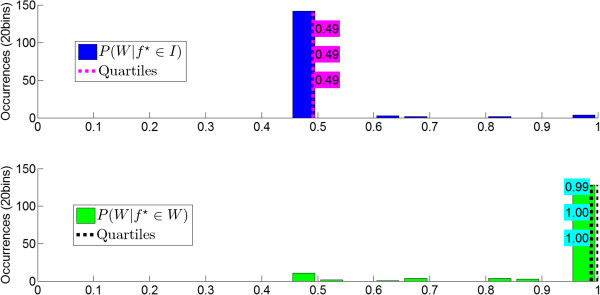
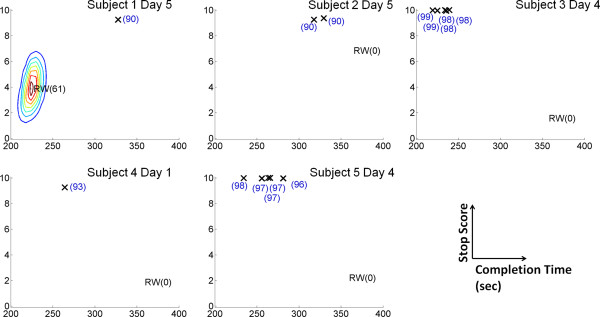
Results: Classification accuracy of idling and walking was estimated offline and ranged from 60.5% (p = 0.0176) to 92.3% (p = 1.36×10-20) across participants and days. Offline analysis revealed that the activation of mid-frontal areas mostly in the μ and low β bands was the most consistent feature for differentiating between idling and walking KMI. In the online task, participants achieved an average performance of 7.4±2.3 successful stops in 273±51 sec. These performances were purposeful, i.e. significantly different from the random walk Monte Carlo simulations (p<0.01), and all but one participant achieved purposeful control within the first day of the experiments. Finally, all participants were able to maintain purposeful control throughout the study, and their online performances improved over time.
Conclusions: The results of this study demonstrate that SCI participants can purposefully operate a self-paced BCI walking simulator to complete a goal-oriented ambulation task. The operation of the proposed BCI system requires short training, is intuitive, and robust against participant-to-participant and day-to-day neurophysiological variations. These findings indicate that BCI-controlled lower extremity prostheses for gait rehabilitation or restoration after SCI may be feasible in the future.
Figures
References
-
- Argo Medical Technologies Ltd. Restoring Upright Mobility. 2010. Yokneam Ilit, Israel. [ http://rewalk.com/]
-
- Harkema S, Gerasimenko Y, Hodes J, Burdick J, Angeli C, Chen Y, Ferreira C, Willhite A, Rejc E, Grossman RG, Edgerton VR. Effect of epidural stimulation of the lumbosacral spinal cord on voluntary movement, standing, and assisted stepping after motor complete paraplegia: a case study. Lancet. 2011;377(9781):1938–1947. doi: 10.1016/S0140-6736(11)60547-3. - DOI - PMC - PubMed
-
- Schmitt JK, Schroeder DL. In: Spinal Cord Medicine - Principles and Practice. Lin VW CardenasDDCutter NC, editor. New York: Demos Medical Publishing; 2003. Endocrine and metabolic consequences of spinal cord injuries; pp. 221–235.
-
- Sabharwal S. In: Spinal Cord Medicine - Principles and Practice. Lin VWCardenas, editor. New York: Demos Medical Publishing; 2003. Cardiovascular dysfunction in spinal cord disorders; pp. 179–192.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
