

Diffusion-weighted imaging of orbital masses: multi-institutional data support a 2-ADC threshold model to categorize lesions as benign, malignant, or indeterminate
- PMID: 23868150
- PMCID: PMC4138308
- DOI: 10.3174/ajnr.A3619
Diffusion-weighted imaging of orbital masses: multi-institutional data support a 2-ADC threshold model to categorize lesions as benign, malignant, or indeterminate
Abstract
Background and purpose: DWI has been increasingly used to characterize orbital masses and provides quantitative information in the form of the ADC, but studies of DWI of orbital masses have shown a range of reported sensitivities, specificities, and optimal threshold ADC values for distinguishing benign from malignant lesions. Our goal was to determine the optimal use of DWI for imaging orbital masses through aggregation of data from multiple centers.
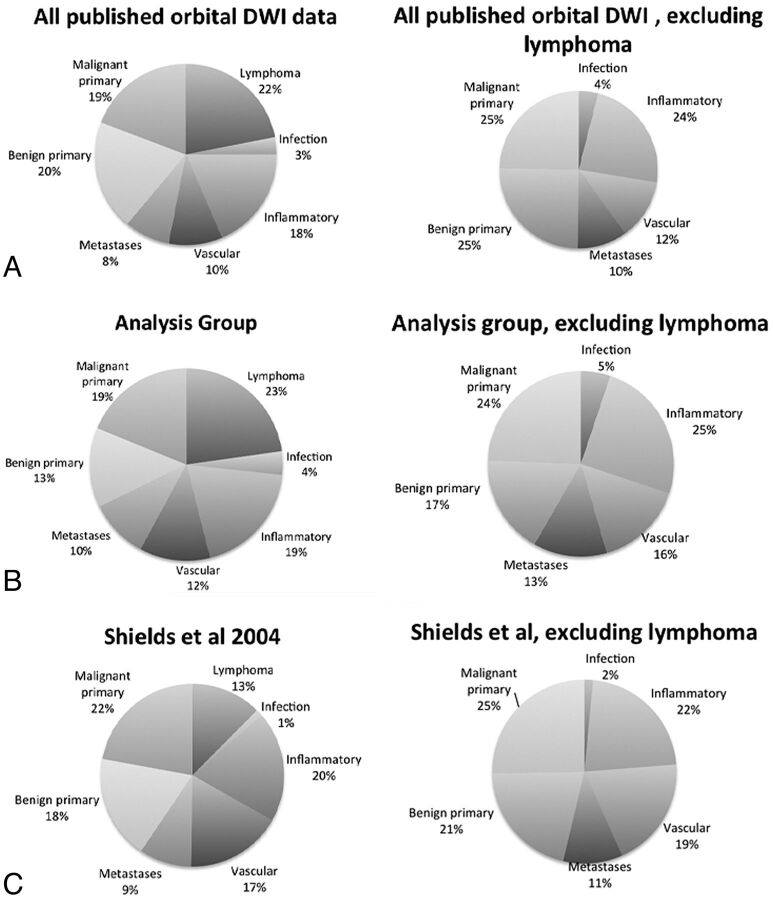
Materials and methods: Source data from 3 previous studies of orbital mass DWI were aggregated, and additional published data points were gathered. Receiver operating characteristic analysis was performed to determine the sensitivity, specificity, and optimal ADC thresholds for distinguishing benign from malignant masses.
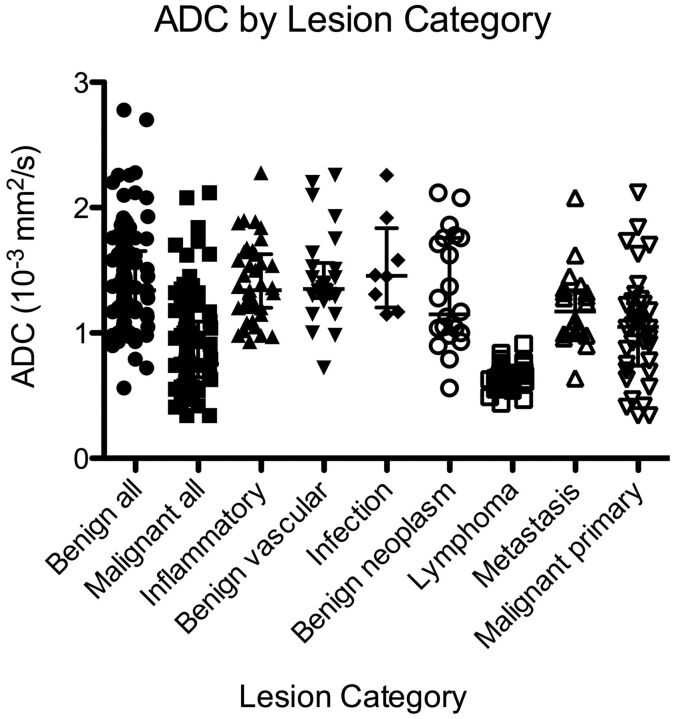
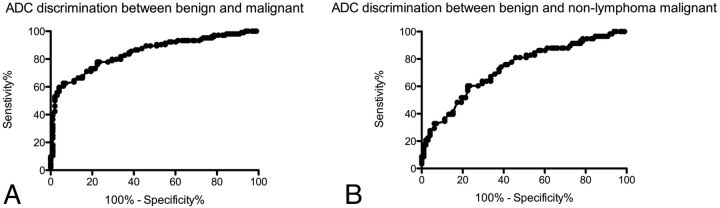
Results: There was no single ADC threshold that characterized orbital masses as benign or malignant with high sensitivity and specificity. An ADC of less than 0.93 × 10(-3) mm(2)/s was more than 90% specific for malignancy, and an ADC of less than 1.35 × 10(-3) mm(2)/s was more than 90% sensitive for malignancy. With these 2 thresholds, 33% of this cohort could be characterized as "likely malignant," 29% as "likely benign," and 38% as "indeterminate."
Conclusions: No single ADC threshold is highly sensitive and specific for characterizing orbital masses as benign or malignant. If we used 2 thresholds to divide these lesions into 3 categories, however, a majority of orbital masses can be characterized with >90% confidence.
Figures
References
-
- Shields J, Shields C, Scartozzi R. Survey of 1264 patients with orbital tumors and simulating lesions. 1. The 2002 Montgomery Lecture, part 1. Ophthalmology 2004;111:997–1008 - PubMed
-
- Mafee M, Karimi A, Shah J, et al. . Anatomy and pathology of the eye: role of MR imaging and CT. Neuroimaging Clin North Am 2005;15:23–47 - PubMed
-
- Mafee MF, Edward DP, Koeller KK, et al. . Lacrimal gland tumors and simulating lesions: clinicopathologic and MR imaging features. Radiol Clin North Am 1999;37:219–39, xii - PubMed
-
- Mafee MF, Goodwin J, Dorodi S. Optic nerve sheath meningiomas: role of MR imaging. Radiol Clin North Am 1999;37:37–58, ix - PubMed
-
- Mafee MF, Dorodi S, Pai E. Sarcoidosis of the eye, orbit, and central nervous system: role of MR imaging. Radiol Clin North Am 1999;37:73–87, x. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical