

4D-CT for preoperative localization of abnormal parathyroid glands in patients with hyperparathyroidism: accuracy and ability to stratify patients by unilateral versus bilateral disease in surgery-naive and re-exploration patients
- PMID: 23868155
- PMCID: PMC7966477
- DOI: 10.3174/ajnr.A3615
4D-CT for preoperative localization of abnormal parathyroid glands in patients with hyperparathyroidism: accuracy and ability to stratify patients by unilateral versus bilateral disease in surgery-naive and re-exploration patients
Abstract
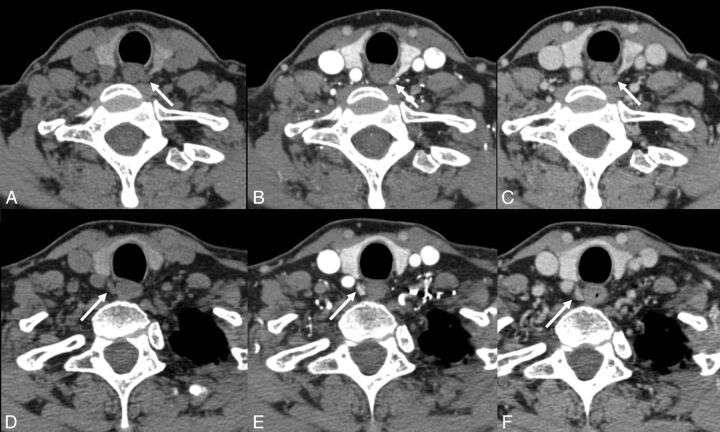
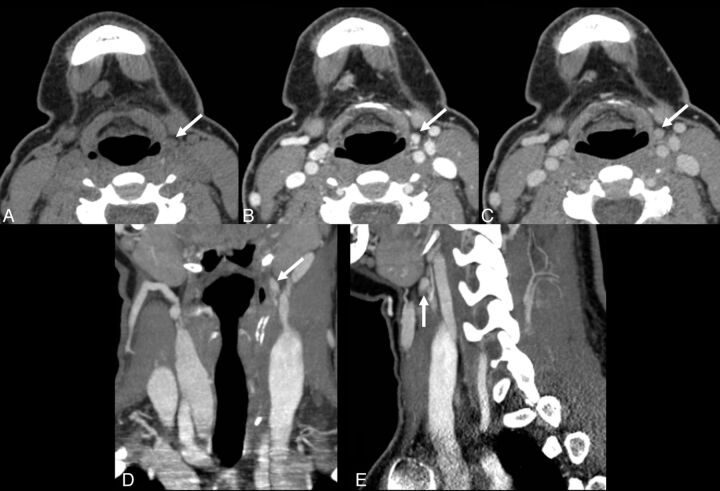
Background and purpose: 4D-CT is an emerging technique that uses high-resolution images, multiplanar reformats, and perfusion characteristics to identify abnormal parathyroid glands in patients with hyperparathyroidism. This study evaluates the accuracy of 4D-CT for localization and lateralization of abnormal parathyroid glands in preoperative planning for minimally invasive parathyroidectomy vs bilateral neck exploration at a tertiary referral center.
Materials and methods: Radiology, pathology, and operative reports were retrospectively reviewed for 208 patients with hyperparathyroidism who underwent 4D-CT and parathyroid surgery between May 2008 and January 2012. 4D-CT performance in localizing side and site was determined by use of surgical and pathologic findings as a reference.
Results: Of 208 patients, 155 underwent initial surgery and 53 underwent re-exploration parathyroid surgery. No lesions were found in 8 patients (3.8%). A total of 284 lesions were found in 200 patients; 233 were correctly localized by 4D-CT (82.0%). Of the 200 patients with parathyroid lesions, 146 underwent unilateral and 54 bilateral neck exploration. 4D-CT correctly identified unilateral vs bilateral disease in 179 (89.5%) of 200. 4D-CT correctly localized parathyroid lesions in 126 of the unilateral cases (86.3%). In the re-exploration cohort, 4D-CT correctly identified unilateral vs bilateral disease in 46 (95.8%) of 48. There was no statistically significant difference in subgroups stratified by surgery type (primary or subsequent) and number of scan phases (3 or 4) (P > .56).
Conclusions: 4D-CT leverages modern high-resolution CT scanning and dynamic contrast enhancement to localize abnormal parathyroid glands in patients with hyperparathyroidism of any cause and can be used for planning minimally invasive parathyroidectomy vs bilateral neck exploration.
Figures
References
-
- The American Association of Clinical Endocrinologists and the American Association of Endocrine Surgeons position statement on the diagnosis and management of primary hyperparathyroidism. Endocr Pract 2005;11:49–54 - PubMed
-
- Fraser WD. Hyperparathyroidism. Lancet 2009;374:145–58 - PubMed
-
- Tominaga Y, Tanaka Y, Sato K, et al. . Histopathology, pathophysiology, and indications for surgical treatment of renal hyperparathyroidism. Semin Surg Oncol 1997;13:78–86 - PubMed
-
- Greene AB, Butler RS, McIntyre S, et al. . National trends in parathyroid surgery from 1998 to 2008: a decade of change. J Am Coll Surg 2009;209:332–43 - PubMed
-
- Udelsman R, Lin Z, Donovan P. The superiority of minimally invasive parathyroidectomy based on 1650 consecutive patients with primary hyperparathyroidism. Ann Surg 2011;253:585–91 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources