

Association of plasma uric acid with ischaemic heart disease and blood pressure: mendelian randomisation analysis of two large cohorts
- PMID: 23869090
- PMCID: PMC3715134
- DOI: 10.1136/bmj.f4262
Association of plasma uric acid with ischaemic heart disease and blood pressure: mendelian randomisation analysis of two large cohorts
Abstract
Objectives: To assess the associations between both uric acid levels and hyperuricaemia, with ischaemic heart disease and blood pressure, and to explore the potentially confounding role of body mass index.
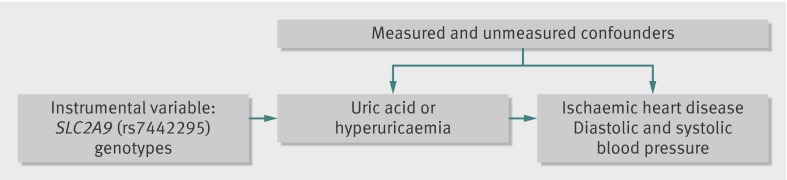
Design: Mendelian randomisation analysis, using variation at specific genes (SLC2A9 (rs7442295) as an instrument for uric acid; and FTO (rs9939609), MC4R (rs17782313), and TMEM18 (rs6548238) for body mass index).
Setting: Two large, prospective cohort studies in Denmark.
Participants: We measured levels of uric acid and related covariables in 58,072 participants from the Copenhagen General Population Study and 10,602 from the Copenhagen City Heart Study, comprising 4890 and 2282 cases of ischaemic heart disease, respectively.
Main outcome: Blood pressure and prospectively assessed ischaemic heart disease.
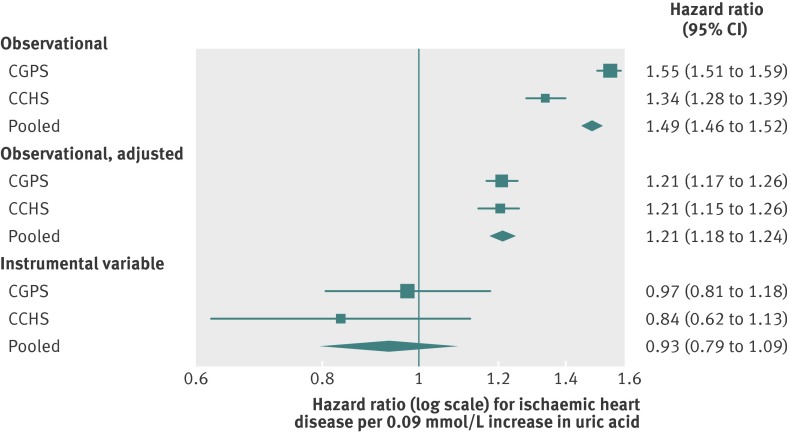
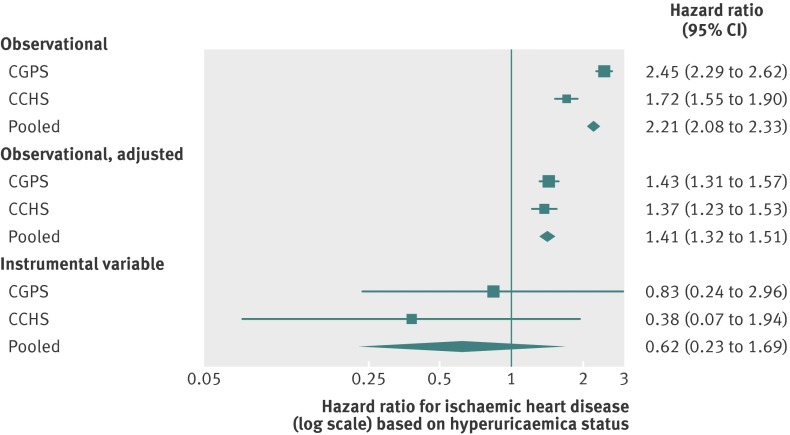
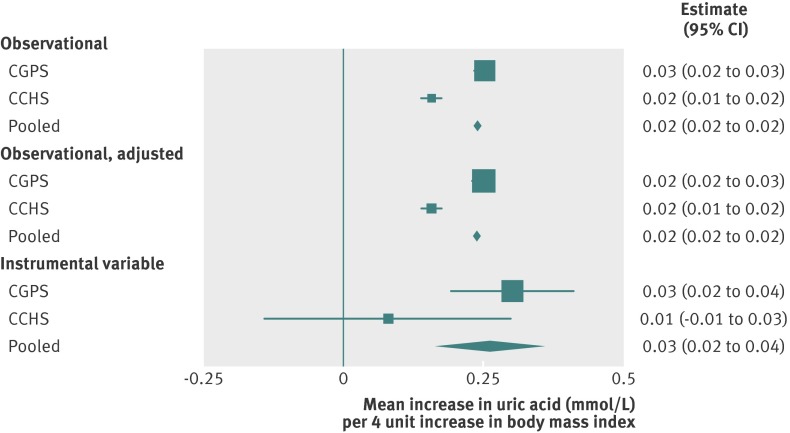
Results: Estimates confirmed known observational associations between plasma uric acid and hyperuricaemia with risk of ischaemic heart disease and diastolic and systolic blood pressure. However, when using genotypic instruments for uric acid and hyperuricaemia, we saw no evidence for causal associations between uric acid, ischaemic heart disease, and blood pressure. We used genetic instruments to investigate body mass index as a potentially confounding factor in observational associations, and saw a causal effect on uric acid levels. Every four unit increase of body mass index saw a rise in uric acid of 0.03 mmol/L (95% confidence interval 0.02 to 0.04), and an increase in risk of hyperuricaemia of 7.5% (3.9% to 11.1%).
Conclusion: By contrast with observational findings, there is no strong evidence for causal associations between uric acid and ischaemic heart disease or blood pressure. However, evidence supports a causal effect between body mass index and uric acid level and hyperuricaemia. This finding strongly suggests body mass index as a confounder in observational associations, and suggests a role for elevated body mass index or obesity in the development of uric acid related conditions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Ethical approval: The studies were approved by the Danish ethical committees and Herlev Hospital, Copenhagen University Hospital (100.2039/91 and 01- 144/01, Copenhagen and Frederiksberg committee).
Data sharing: Additional data regarding technical details, statistical code, and derivative data is available from the principal investigator at
Figures

Comment in
-
Asociación de la uricemia con la cardiopatía isquémica y la presión arterial: análisis mediante aleatorización mendeliana de 2 grandes cohortes.Rev Clin Esp (Barc). 2014 Jan-Feb;214(1):48. doi: 10.1016/j.rce.2013.08.003. Rev Clin Esp (Barc). 2014. PMID: 24624425 Spanish. No abstract available.
References
-
- Phay JE, Hussain HB, Moley JF. Cloning and expression analysis of a novel member of the facilitative glucose transporter family, SLC2A9 (GLUT9). Genomics 2000;66:217-20. - PubMed
-
- Vitart V, Rudan I, Hayward C, Gray NK, Floyd J, Palmer CNA, et al. SLC2A9 is a newly identified urate transporter influencing serum urate concentration, urate excretion and gout. Nat Genet 2008;40:437-42. - PubMed
-
- Wu X, Muzny DM, Chi Lee C, Thomas Caskey C. Two independent mutational events in the loss of urate oxidase during hominoid evolution. J Mol Evol 1992;34:78-84. - PubMed
-
- Nesse RM, Williams GC. Evolution and healing: the new science of Darwinian medicine. Phoenix, 1996.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources