

Surgical anatomy of the upper eyelid relating to upper blepharoplasty or blepharoptosis surgery
- PMID: 23869256
- PMCID: PMC3713284
- DOI: 10.5115/acb.2013.46.2.93
Surgical anatomy of the upper eyelid relating to upper blepharoplasty or blepharoptosis surgery
Abstract
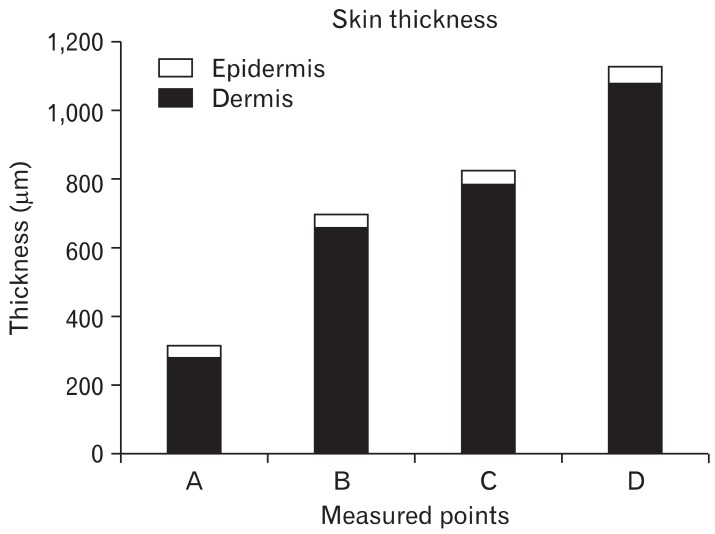
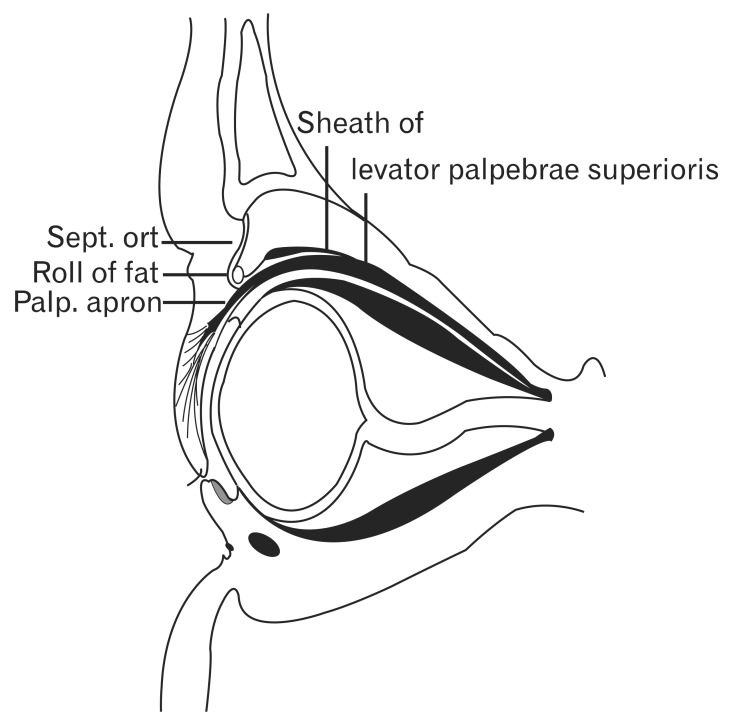
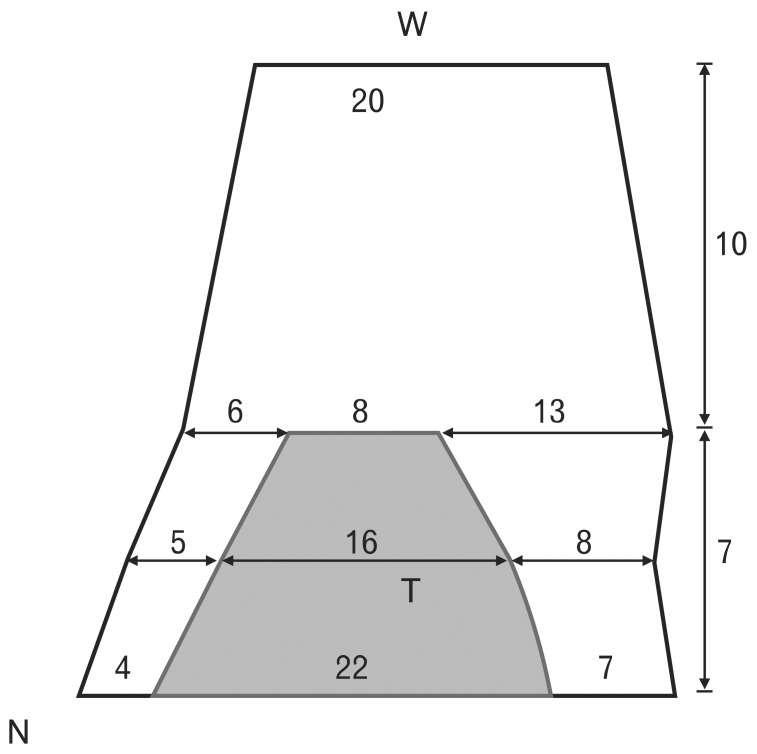
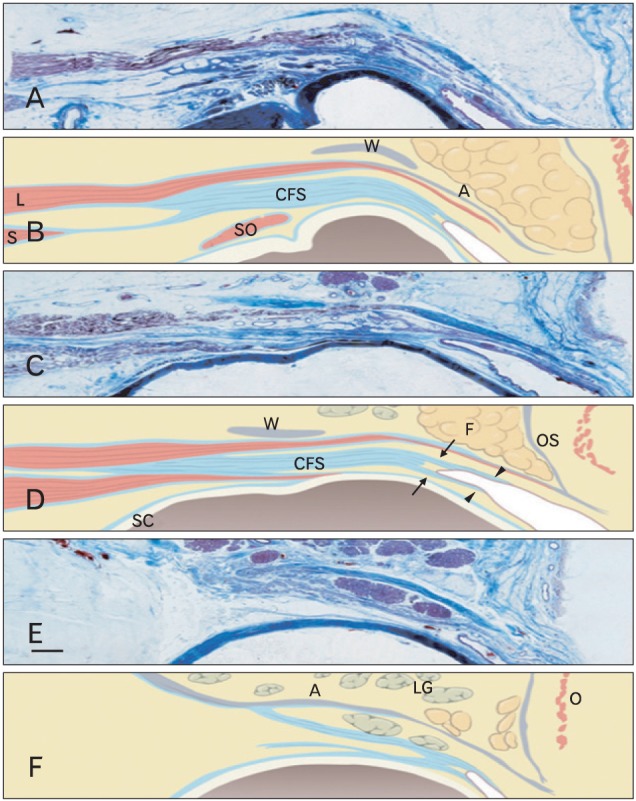
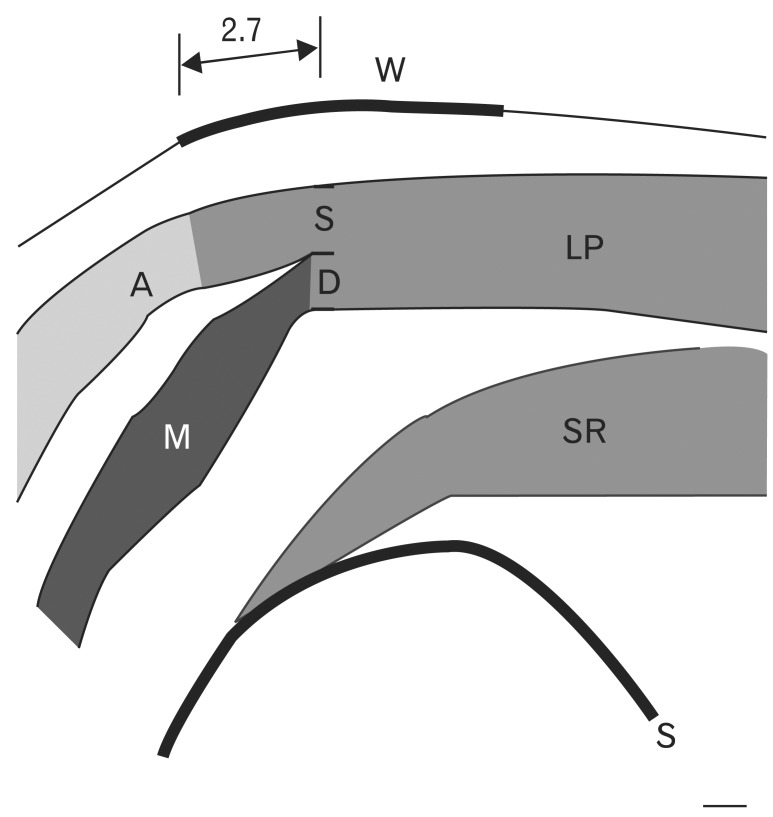
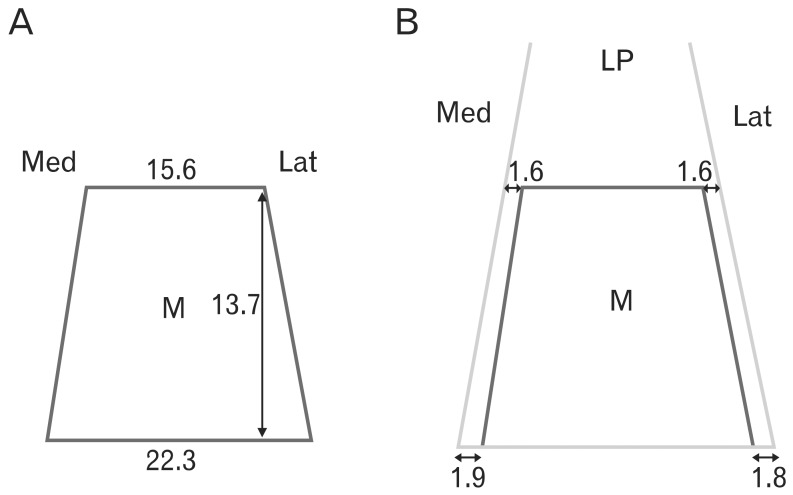
Eyelid anatomy, including thickness measurements, was examined in numerous age groups. The thickest part of the upper eyelid is just below the eyebrow (1.127±238 µm), and the thinnest near the ciliary margin (320±49 µm). The thickness of skin at 7 mm above the eyelashes was 860±305 µm. The results revealed no significant differences among the age groups. Fast fibers (87.8±3.7%) occupied a significantly larger portion of the orbicularis oculi muscle (OOM) than nonfast fibers (12.2±3.7%). The frontalis muscle passed through and was inserted into the bundles of the OOM on the superior border of the eyebrow at the middle and medial portions of the upper eyelid. Laterally, the frontalis muscle inserted about 0.5 cm below the superior border of the eyebrow. Fast fibers occupied a significantly larger portion of the OOM than did non-fast fibers. The oculomotor nerve ends that extend forward to the distal third of the levator muscle are exposed and vulnerable to local anesthetics and may be numbed during blepharoplasty. The orbital septum consists of 2 layers. The outer layer of loose connective tissue descends to interdigitate with the levator aponeurosis and disperses inferiorly. The inner layer follows the outer layer, then reflects and continues posteriorly with the levator sheath. Widths of the tarsal plate at its lower border, mid-height, and upper border were 21.8±1.8, 16.2±1.6, and 8.3±1.0 mm, respectively. The widths of the levator aponeurosis were 32.0±2.2, 29.2±3.5, and 27.2±3.9 mm, respectively. Below the levator, the "conjoint fascial sheath" (CFS) is attached to the conjunctival fornix. The CFS was 12.2±2.0 mm anteroposterior length and 1.1±0.1 mm thick. The shape was equilateral trapezoid with a longer base anteriorly. The superior palpebral muscle was trapezoidal. The lengths of its sides were 15.58±1.82 and 22.30±5.25 mm, and its height was 13.70±2.74 mm. The width of the levator aponeurosis was approximately 4 mm wider than the superior palpebral muscle.
Keywords: Anatomy and histology; Blepharoplasty; Blepharoptosis; Eyelids.
Figures

References
-
- Barker DE. Skin thickness in the human. Plast Reconstr Surg (1946) 1951;7:115–116. - PubMed
-
- Lee Y, Hwang K. Skin thickness of Korean adults. Surg Radiol Anat. 2002;24:183–189. - PubMed
-
- Hwang K, Kim DJ, Hwang SH. Thickness of Korean upper eyelid skin at different levels. J Craniofac Surg. 2006;17:54–56. - PubMed
-
- Gonzalez-Ulloa M, Flores ES. Senility of the face: basic study to understand its causes and effects. Plast Reconstr Surg. 1965;36:239–246. - PubMed
-
- Hykin PG, Bron AJ. Age-related morphological changes in lid margin and meibomian gland anatomy. Cornea. 1992;11:334–342. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical