

National trends in pancreaticoduodenal trauma: interventions and outcomes
- PMID: 23869407
- PMCID: PMC3945854
- DOI: 10.1111/hpb.12125
National trends in pancreaticoduodenal trauma: interventions and outcomes
Abstract
Objectives: Pancreaticoduodenal trauma (PDT) is associated with substantial mortality and morbidity. In this study, contemporary trends were analysed using national data.
Methods: The Nationwide Inpatient Sample for 1998-2009 was queried for patients with PDT. Interventions including any operation (Any-Op) and pancreas-specific surgery (PSURG) were identified. Trends in treatment and outcomes were determined [complications, length of stay (LoS), mortality] for the Any-Op, PSURG and non-operative (Non-Op) groups. Analyses included chi-squared tests, Cochran-Armitage trend tests and logistic regression.
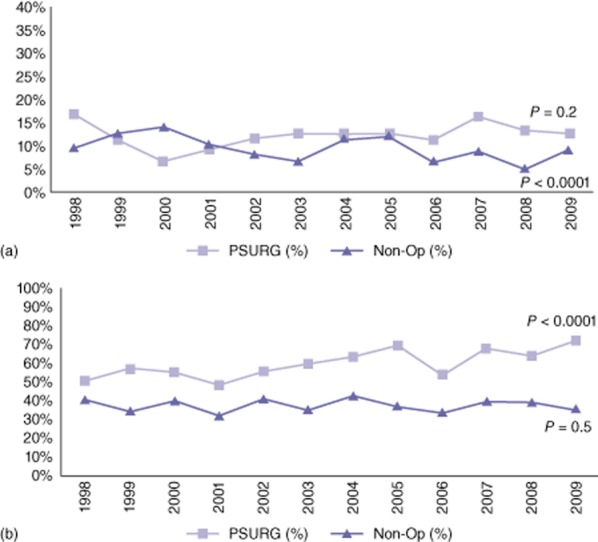
Results: A total of 27 216 patients (nationally weighted) with PDT were identified. Over time, the frequency of PDT increased by 8.3%, whereas the proportion of patients submitted to PSURG declined (from 21.7% to 19.8%; P = 0.0004) and the percentage of patients submitted to non-operative management increased (from 56.7% to 59.1%; P = 0.01). In the Non-Op group, mortality decreased from 9.7% to 8.6% (P < 0.001); morbidity and LoS remained unchanged at ∼40% and ∼12 days, respectively. In the PSURG group, mortality remained stable at ∼15%, complications increased from 50.2% to 71.8% (P < 0.0001) and LoS remained stable at ∼21 days. For all PDT patients, significant independent predictors of mortality included: the presence of combined pancreatic and duodenal injuries; penetrating trauma, and age >50 years. Having any operation (Any-Op) was associated with mortality, but PSURG was not a predictor of death.
Conclusions: The utilization of operations for PDT has declined without affecting mortality, but operative morbidity increased significantly over the 12 years to 2009. The development of an evidence-based approach to invasive manoeuvres and an early multidisciplinary approach involving pancreatic surgeons may improve outcomes in patients with these morbid injuries.
© 2013 International Hepato-Pancreato-Biliary Association.
Figures
References
-
- Lin BC, Fang JF, Wong YC, Liu NJ. Blunt pancreatic trauma and pseudocyst: management of major pancreatic duct injury. Injury. 2007;38:588–593. - PubMed
-
- Asensio JA, Demetriades D, Hanpeter DE, Gambaro E, Chahwan S. Management of pancreatic injuries. Curr Probl Surg. 1999;36:325–419. - PubMed
-
- Johnson MA, Rajendran S, Balachandar TG, Kannan DG, Jeswanth S, Ravichandran P, et al. Central pancreatectomy for benign pancreatic pathology/trauma: is it a reasonable pancreas-preserving conservative surgical strategy alternative to standard major pancreatic resection? ANZ J Surg. 2006;76:987–995. - PubMed
-
- Patton JH, Jr, Lyden SP, Croce MA, Pritchard FE, Minard G, Kudsk KA, et al. Pancreatic trauma: a simplified management guideline. J Trauma. 1997;43:234–239. - PubMed
-
- Antonacci N, Di Saverio S, Ciaroni V, Biscardi A, Giugni A, Cancellieri F, et al. Prognosis and treatment of pancreaticoduodenal traumatic injuries: which factors are predictors of outcome? J Hepatobiliary Pancreat Sci. 2011;18:195–201. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
