

Medical virology of hepatitis B: how it began and where we are now
- PMID: 23870415
- PMCID: PMC3729363
- DOI: 10.1186/1743-422X-10-239
Medical virology of hepatitis B: how it began and where we are now
Abstract
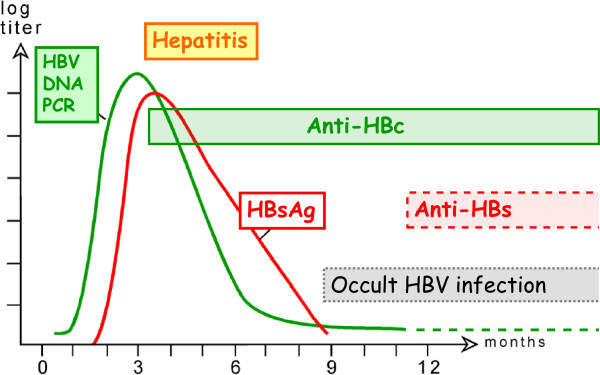
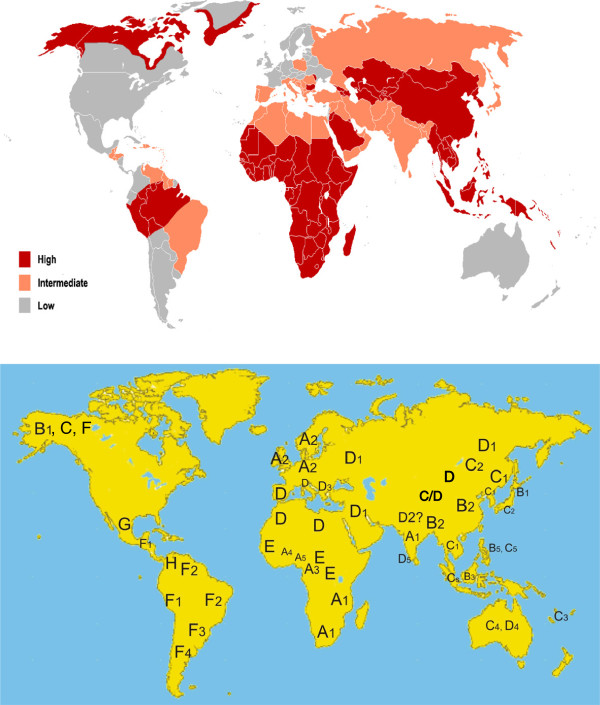
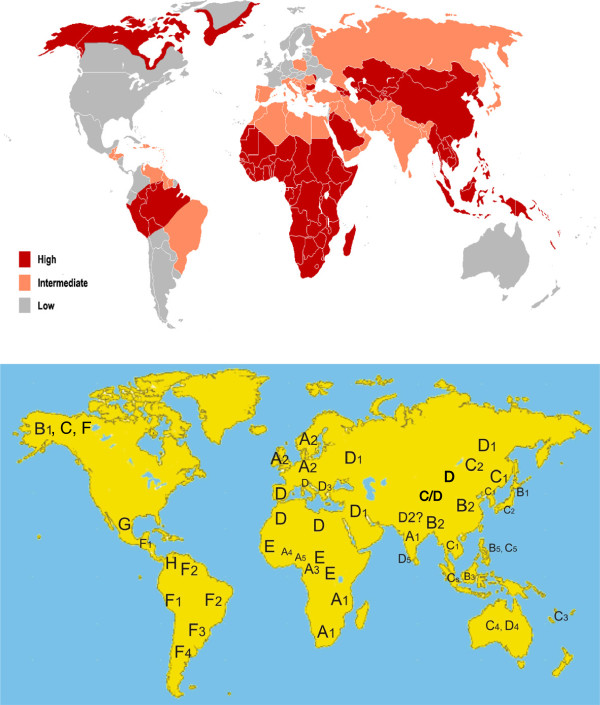
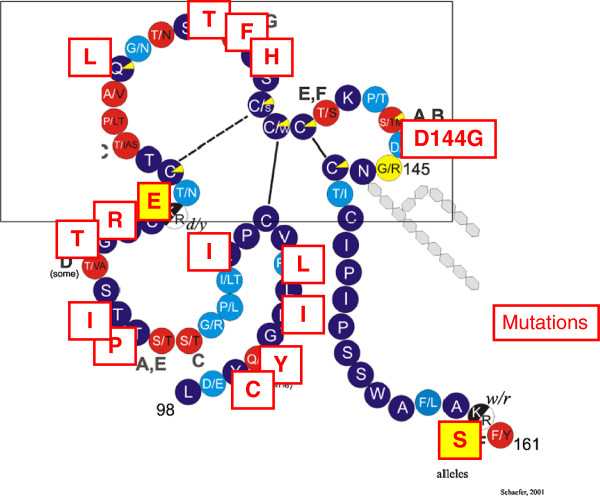
Infection with hepatitis B virus (HBV) may lead to acute or chronic hepatitis. HBV infections were previously much more frequent but there are still 240 million chronic HBV carriers today and ca. 620,000 die per year from the late sequelae liver cirrhosis or hepatocellular carcinoma. Hepatitis B was recognized as a disease in ancient times, but its etiologic agent was only recently identified. The first clue in unraveling this mystery was the discovery of an enigmatic serum protein named Australia antigen 50 years ago by Baruch Blumberg. Some years later this was recognized to be the HBV surface antigen (HBsAg). Detection of HBsAg allowed for the first time screening of inapparently infected blood donors for a dangerous pathogen. The need to diagnose clinically silent HBV infections was a strong driving force in the development of modern virus diagnostics. HBsAg was the first infection marker to be assayed with a highly sensitive radio immune assay. HBV itself was among the first viruses to be detected by assay of its DNA genome and IgM antibodies against the HBV core antigen were the first to be selectively detected by the anti-μ capture assay. The cloning and sequencing of the HBV genome in 1978 paved the way to understand the viral life cycle, and allowed development of efficient vaccines and drugs. Today's hepatitis B vaccine was the first vaccine produced by gene technology. Among the problems that still remain today are the inability to achieve a complete cure of chronic HBV infections, the recognition of occult HBV infections, their potential reactivation and the incomplete protection against escape mutants and heterologous HBV genotypes by HBV vaccines.
Figures
References
-
- Blumberg BS. Hepatitis B - The hunt for a killer virus. Princeton: Princeton University Press; 2002.
-
- Lürmann A. Eine Icterusepidemie. Ber Klin Wochenschr. 1885. pp. 20–23.
-
- Seeff LB, Beebe GW, Hoofnagle JH, Norman JE, Buskell-Bales Z, Waggoner JG, Kaplowitz N, Koff RS, Petrini JL Jr, Schiff ER. et al.A serologic follow-up of the 1942 epidemic of post-vaccination hepatitis in the United States Army. N Engl J Med. 1987;10:965–970. doi: 10.1056/NEJM198704163161601. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
