

Joubert syndrome: congenital cerebellar ataxia with the molar tooth
- PMID: 23870701
- PMCID: PMC3809058
- DOI: 10.1016/S1474-4422(13)70136-4
Joubert syndrome: congenital cerebellar ataxia with the molar tooth
Abstract
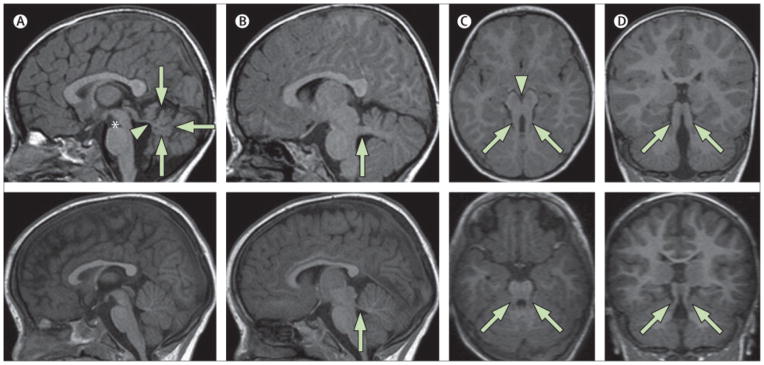
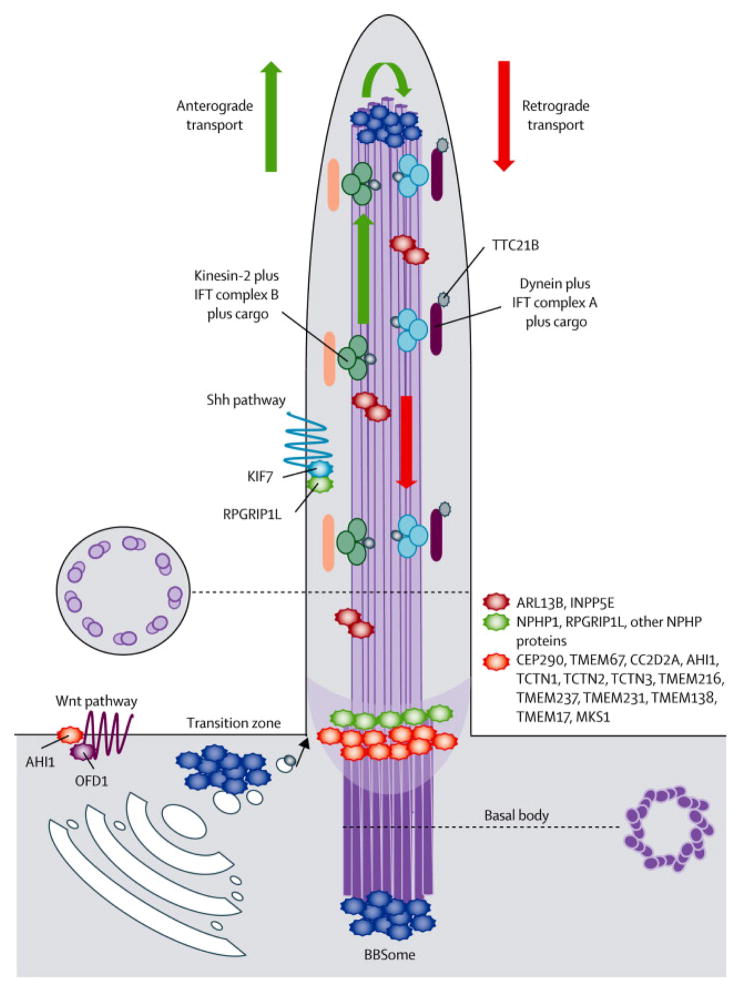
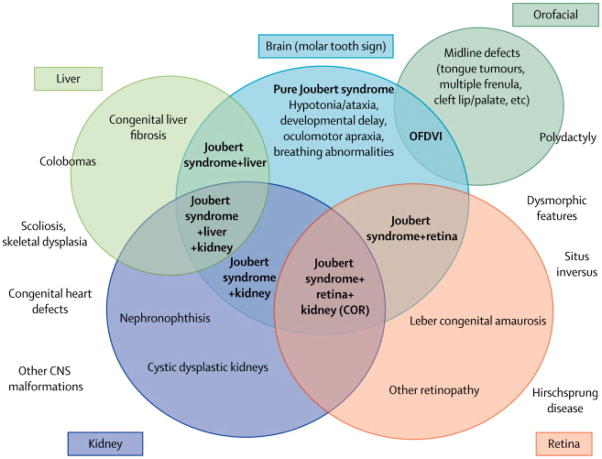
Joubert syndrome is a congenital cerebellar ataxia with autosomal recessive or X-linked inheritance, the diagnostic hallmark of which is a unique cerebellar and brainstem malformation recognisable on brain imaging-the so-called molar tooth sign. Neurological signs are present from the neonatal period and include hypotonia progressing to ataxia, global developmental delay, ocular motor apraxia, and breathing dysregulation. These signs are variably associated with multiorgan involvement, mainly of the retina, kidneys, skeleton, and liver. 21 causative genes have been identified so far, all of which encode for proteins of the primary cilium or its apparatus. The primary cilium is a subcellular organelle that has key roles in development and in many cellular functions, making Joubert syndrome part of the expanding family of ciliopathies. Notable clinical and genetic overlap exists between distinct ciliopathies, which can co-occur even within families. Such variability is probably explained by an oligogenic model of inheritance, in which the interplay of mutations, rare variants, and polymorphisms at distinct loci modulate the expressivity of the ciliary phenotype.
Copyright © 2013 Elsevier Ltd. All rights reserved.
Conflict of interest statement
The authors declare they have no conflict of interest.
Figures
References
-
- Pazour GJ, Bloodgood RA. Targeting proteins to the ciliary membrane. Curr Top Dev Biol. 2008;85:115–49. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
