

Exercise increases age-related penetrance and arrhythmic risk in arrhythmogenic right ventricular dysplasia/cardiomyopathy-associated desmosomal mutation carriers
- PMID: 23871885
- PMCID: PMC3809992
- DOI: 10.1016/j.jacc.2013.06.033
Exercise increases age-related penetrance and arrhythmic risk in arrhythmogenic right ventricular dysplasia/cardiomyopathy-associated desmosomal mutation carriers
Abstract
Objectives: This study sought to determine how exercise influences penetrance of arrhythmogenic right ventricular dysplasia/cardiomyopathy (ARVD/C) among patients with desmosomal mutations.
Background: Although animal models and anecdotal evidence suggest that exercise is a risk factor for ARVD/C, there have been no systematic human studies.
Methods: Eighty-seven carriers (46 male; mean age, 44 ± 18 years) were interviewed about regular physical activity from 10 years of age. The relationship of exercise with sustained ventricular arrhythmia (ventricular tachycardia/ventricular fibrillation [VT/VF]), stage C heart failure (HF), and meeting diagnostic criteria for ARVD/C (2010 Revised Task Force Criteria [TFC]) was studied.
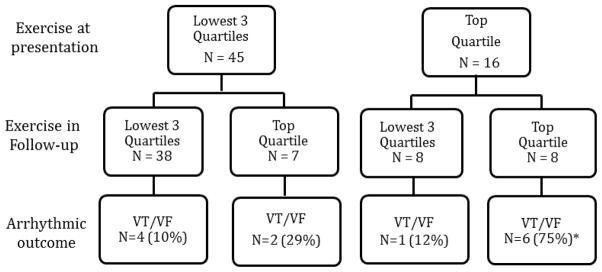
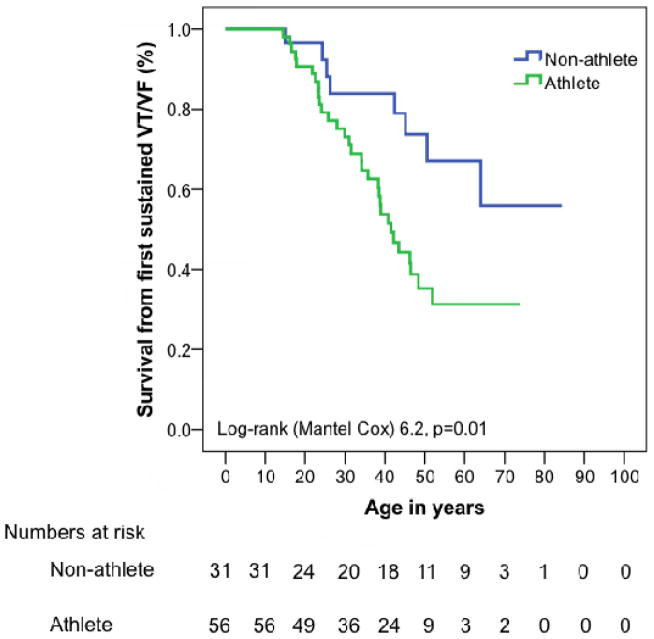
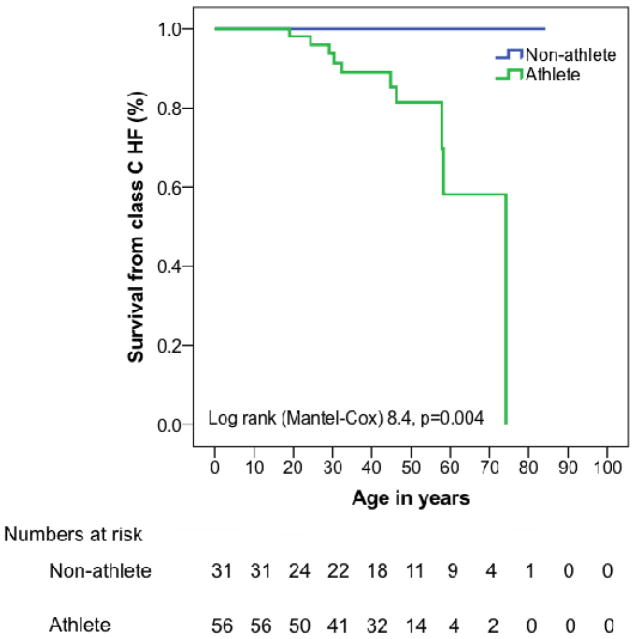
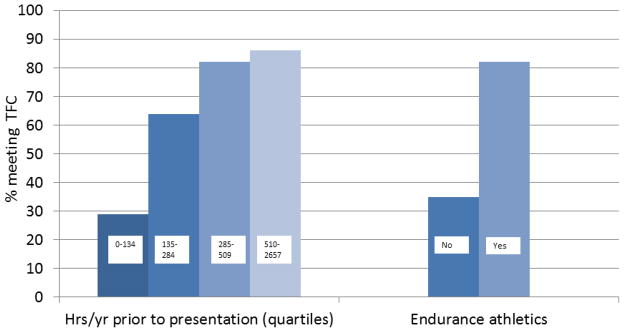
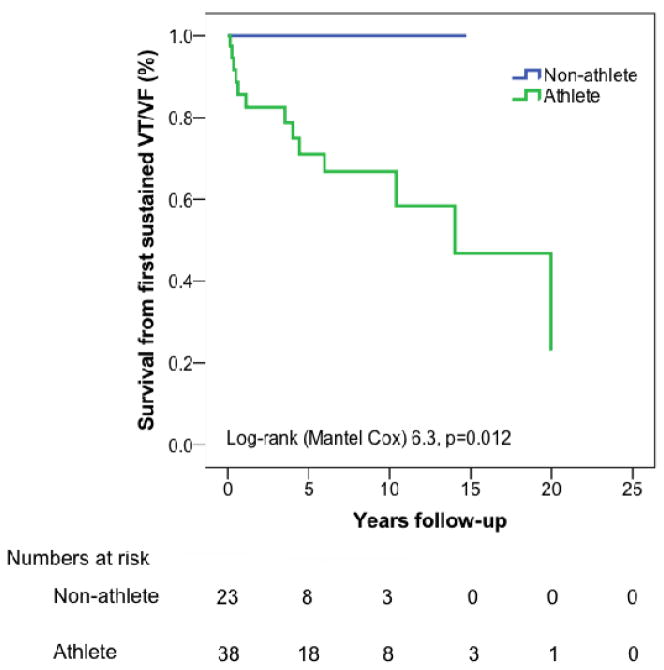
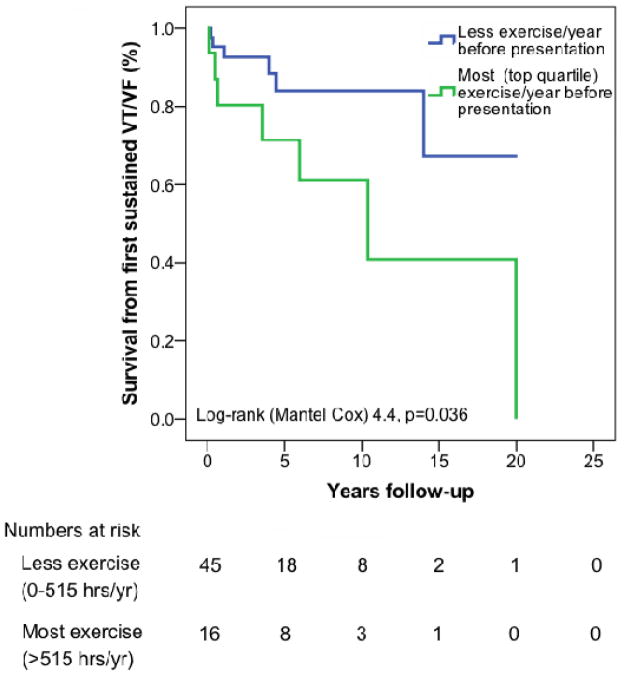
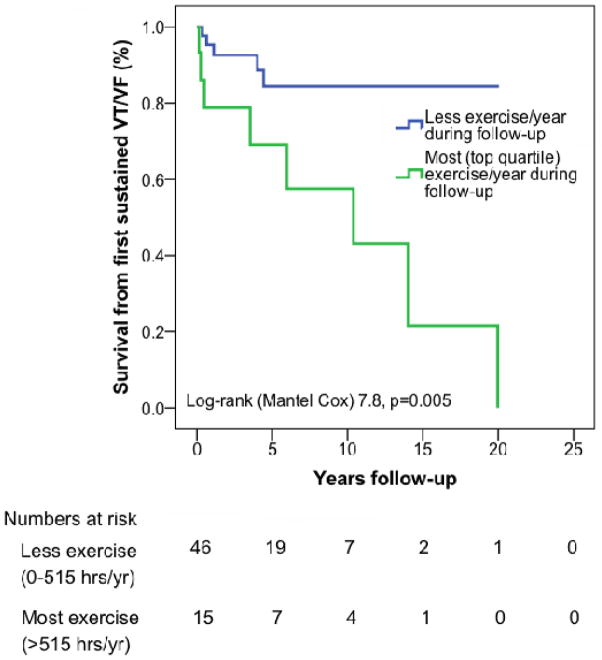
Results: Symptoms developed in endurance athletes (N = 56) at a younger age (30.1 ± 13.0 years vs. 40.6 ± 21.1 years, p = 0.05); they were more likely to meet TFC at last follow-up (82% vs. 35%, p < 0.001) and have a lower lifetime survival free of VT/VF (p = 0.013) and HF (p = 0.004). Compared with those who did the least exercise per year (lowest quartile) before presentation, those in the second (odds ratio [OR]: 6.64, p = 0.013), third (OR: 16.7, p = 0.001), and top (OR: 25.3, p < 0.0001) quartiles were increasingly likely to meet TFC. Among 61 individuals who did not present with VT/VF, the 13 subjects experiencing a first VT/VF event over a mean follow-up of 8.4 ± 6.7 years were all endurance athletes (p = 0.002). Survival from a first VT/VF event was lowest among those who exercised most (top quartile) both before (p = 0.036) and after (p = 0.005) clinical presentation. Among individuals in the top quartile, a reduction in exercise decreased VT/VF risk (p = 0.04).
Conclusions: Endurance exercise and frequent exercise increase the risk of VT/VF, HF, and ARVD/C in desmosomal mutation carriers. These findings support exercise restriction for these patients.
Keywords: (stage C) heart failure; 2010 Revised Task Force Criteria; ARVD/C; CI; ECG; HF; ICD; IQR; OR; RV; TFC; VT/VF; arrhythmogenic right ventricular dysplasia; arrhythmogenic right ventricular dysplasia/cardiomyopathy; cardiomyopathy; confidence interval; electrocardiogram; exercise; heart failure; implantable cardioverter-defibrillator; interquartile range; odds ratio; penetrance; right ventricular; ventricular arrhythmias; ventricular tachycardia/ventricular fibrillation.
Copyright © 2013 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Marcus F, Fontaine G, Guiraudon G, et al. Right ventricular dysplasia: a report of 24 adult cases. Circulation. 1982;65:384–98. - PubMed
-
- Fontaine G. Arrhythmogenic right ventricular dysplasia. Curr Opin Cardiol. 1995;10:16–20. - PubMed
-
- Basso C, Corrado D, Marcus FI, Nava A, Thiene G. Arrhythmogenic right ventricular cardiomyopathy. Lancet. 2009;373:1289–1300. - PubMed
-
- Dalal D, Nasir K, Bomma C, et al. Arrhythmogenic right ventricular dysplasia. Circulation. 2005;112:3823–32. - PubMed
-
- Sen-Chowdhry S, Morgan RD, Chambers JC, McKenna WJ. Arrhythmogenic cardiomyopathy: etiology, diagnosis, and treatment. Annu Rev Med. 2010;61:233–53. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
