

Changes in association between previous therapeutic abortion and preterm birth in Scotland, 1980 to 2008: a historical cohort study
- PMID: 23874161
- PMCID: PMC3706322
- DOI: 10.1371/journal.pmed.1001481
Changes in association between previous therapeutic abortion and preterm birth in Scotland, 1980 to 2008: a historical cohort study
Abstract
Background: Numerous studies have demonstrated that therapeutic termination of pregnancy (abortion) is associated with an increased risk of subsequent preterm birth. However, the literature is inconsistent, and methods of abortion have changed dramatically over the last 30 years. We hypothesized that the association between previous abortion and the risk of preterm first birth changed in Scotland between 1 January 1980 and 31 December 2008.
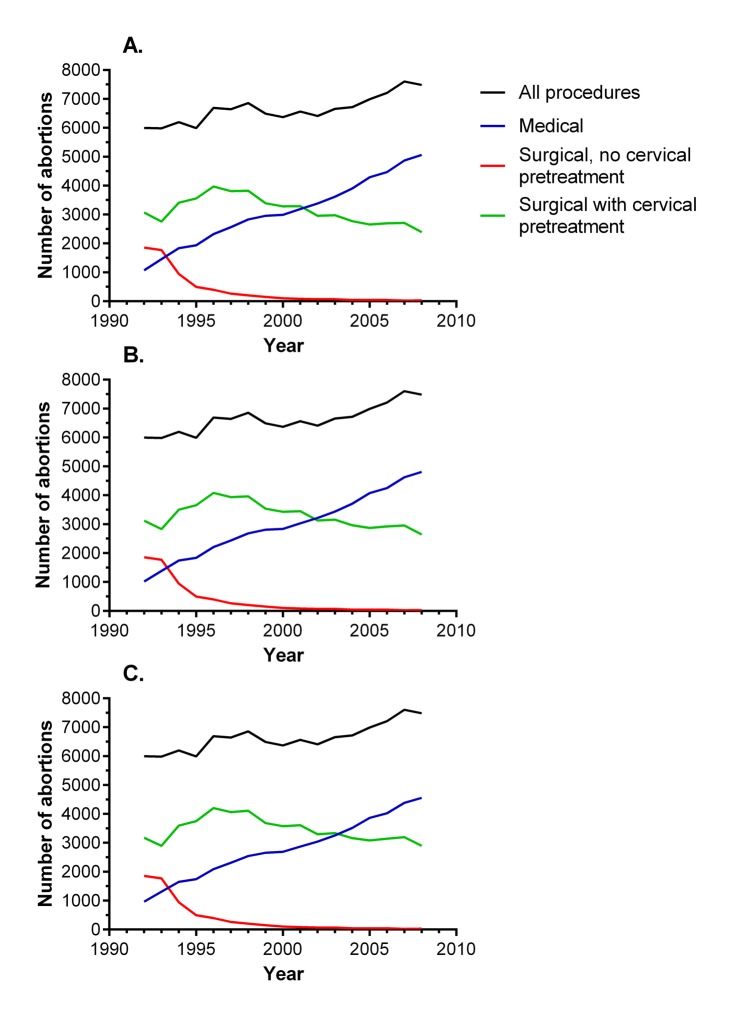
Methods and findings: We studied linked Scottish national databases of births and perinatal deaths. We analysed the risk of preterm birth in relation to the number of previous abortions in 732,719 first births (≥24 wk), adjusting for maternal characteristics. The risk (adjusted odds ratio [95% CI]) of preterm birth was modelled using logistic regression, and associations were expressed for a one-unit increase in the number of previous abortions. Previous abortion was associated with an increased risk of preterm birth (1.12 [1.09-1.16]). When analysed by year of delivery, the association was strongest in 1980-1983 (1.32 [1.21-1.43]), progressively declined between 1984 and 1999, and was no longer apparent in 2000-2003 (0.98 [0.91-1.05]) or 2004-2008 (1.02 [0.95-1.09]). A statistical test for interaction between previous abortion and year was highly statistically significant (p<0.001). Analysis of data for abortions among nulliparous women in Scotland 1992-2008 demonstrated that the proportion that were surgical without use of cervical pre-treatment decreased from 31% to 0.4%, and that the proportion of medical abortions increased from 18% to 68%.
Conclusions: Previous abortion was a risk factor for spontaneous preterm birth in Scotland in the 1980s and 1990s, but the association progressively weakened and disappeared altogether by 2000. These changes were paralleled by increasing use of medical abortion and cervical pre-treatment prior to surgical abortion. Although it is plausible that the two trends were related, we could not test this directly as the data on the method of prior abortions were not linked to individuals in the cohort. However, we speculate that modernising abortion methods may be an effective long-term strategy to reduce global rates of preterm birth.
Conflict of interest statement
GCSS is a member of the Editorial Board of
Figures




References
-
- Sedgh G, Singh S, Shah IH, Ahman E, Henshaw SK, et al. (2012) Induced abortion: incidence and trends worldwide from 1995 to 2008. Lancet 379: 625–632. - PubMed
-
- Shah PS, Zao J (2009) Induced termination of pregnancy and low birthweight and preterm birth: a systematic review and meta-analyses. BJOG 116: 1425–1442. - PubMed
-
- Royal College of Obstetricians and Gynaecologists (2011) RCOG evidence-based clinical guideline no 7: the care of women requesting induced abortion. London: Royal College of Obstetricians and Gynaecologists.
-
- Bygdeman M (1992) Prostaglandin analogues and their uses. Baillieres Clin Obstet Gynaecol 6: 893–903. - PubMed
-
- Baird DT (2001) Antigestogens: the holy grail of contraception. Reprod Fertil Dev 13: 723–728. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
