

Radiation-induced temporal lobe injury for nasopharyngeal carcinoma: a comparison of intensity-modulated radiotherapy and conventional two-dimensional radiotherapy
- PMID: 23874422
- PMCID: PMC3707870
- DOI: 10.1371/journal.pone.0067488
Radiation-induced temporal lobe injury for nasopharyngeal carcinoma: a comparison of intensity-modulated radiotherapy and conventional two-dimensional radiotherapy
Abstract
Background: To compare the radiation-induced temporal lobe injury (TLI) in patients with nasopharyngeal carcinoma (NPC) treated with intensity-modulated radiotherapy (IMRT) or two-dimensional conventional radiotherapy (2D-CRT).
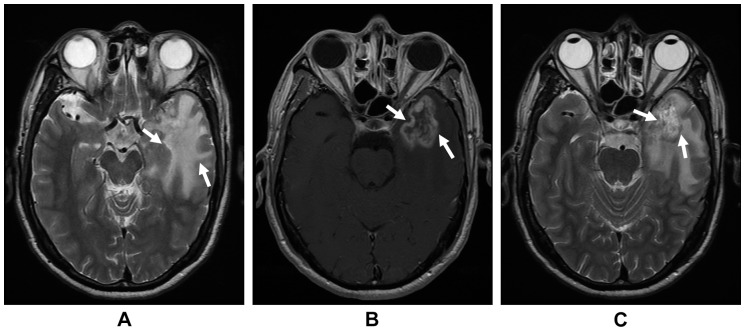
Patients and methods: 1276 cases of NPC treated with IMRT or 2D-CRT were retrospectively reviewed. A diagnosis of TLI was made on follow-up magnetic resonance imaging (MRI).
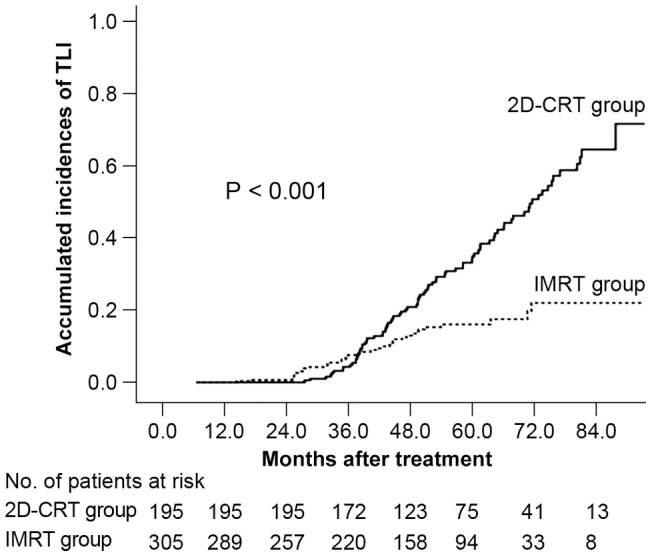
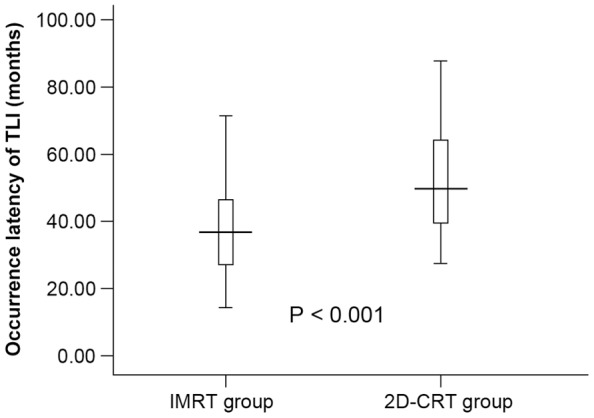
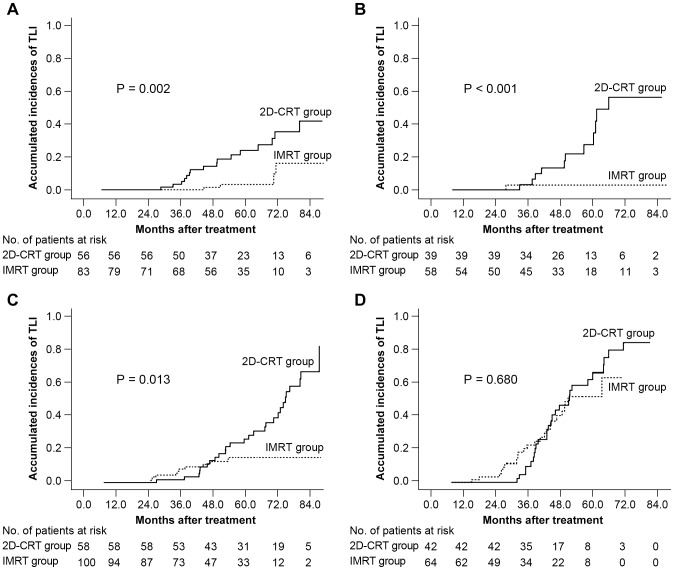
Results: The crude incidence of TLI was 7.5% and 10.8% (P = 0.048), and the actuarial 5-year incidence was 16% and 34.9% (P<0.001) for the IMRT and 2D-CRT groups, respectively. Multivariate analysis revealed both T stage (P<0.001) and radiation technique (P<0.001) as independent predictors. Patients with T1, T2 and T3 disease had a significantly higher risk when treated with 2D-CRT (P = 0.005, 0.016, <0.001, respectively). This trend was not evident for T4 patients (P = 0.680). The 2D-CRT group had a longer latency for the development of TLI (P<0.001). Those with T4 disease had a shorter median time to TLI (P = 0.006, 0.042, <0.001 when compared with T1, T2 and T3, respectively).
Conclusions: IMRT is superior to 2DRT for the management of T1-T3 NPC in terms of sparing the temporal lobe. The high incidence of TLI in T4 disease needs to be addressed.
Conflict of interest statement
Figures
References
-
- Jemal A, Bray F (2011) Center MM, Ferlay J, Ward E, et al (2011) Global cancer statistics. CA Cancer J Clin 61: 69–90. - PubMed
-
- Lee AW, Ng SH, Ho JH, Tse VK, Poon YF, et al. (1988) Clinical diagnosis of late temporal lobe necrosis following radiation therapy for nasopharyngeal carcinoma. Cancer 61: 1535–42. - PubMed
-
- Lee AW, Sze WM, Fowler JF, Chappell R, Leung SF, et al. (1999) Caution on the use of altered fractionation for nasopharyngeal carcinoma. Radiother Oncol 52(3): 207–11. - PubMed
-
- Cheung MC, Chan AS, Law SC, Chan JH, Tse VK (2003) Impact of radionecrosis on cognitive dysfunction in patients after radiotherapy for nasopharyngeal carcinoma. Cancer 97(8): 2019–26. - PubMed
-
- Lee AW, Law SC, Ng SH, Chan DK, Poon YF, et al. (1992) Retrospective analysis of nasopharyngeal carcinoma treated during 1976–1985: Late complications following megavoltage irradiation. Br J Radiol 65: 918–928. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
