

Effects of white matter injury on resting state fMRI measures in prematurely born infants
- PMID: 23874510
- PMCID: PMC3706620
- DOI: 10.1371/journal.pone.0068098
Effects of white matter injury on resting state fMRI measures in prematurely born infants
Abstract
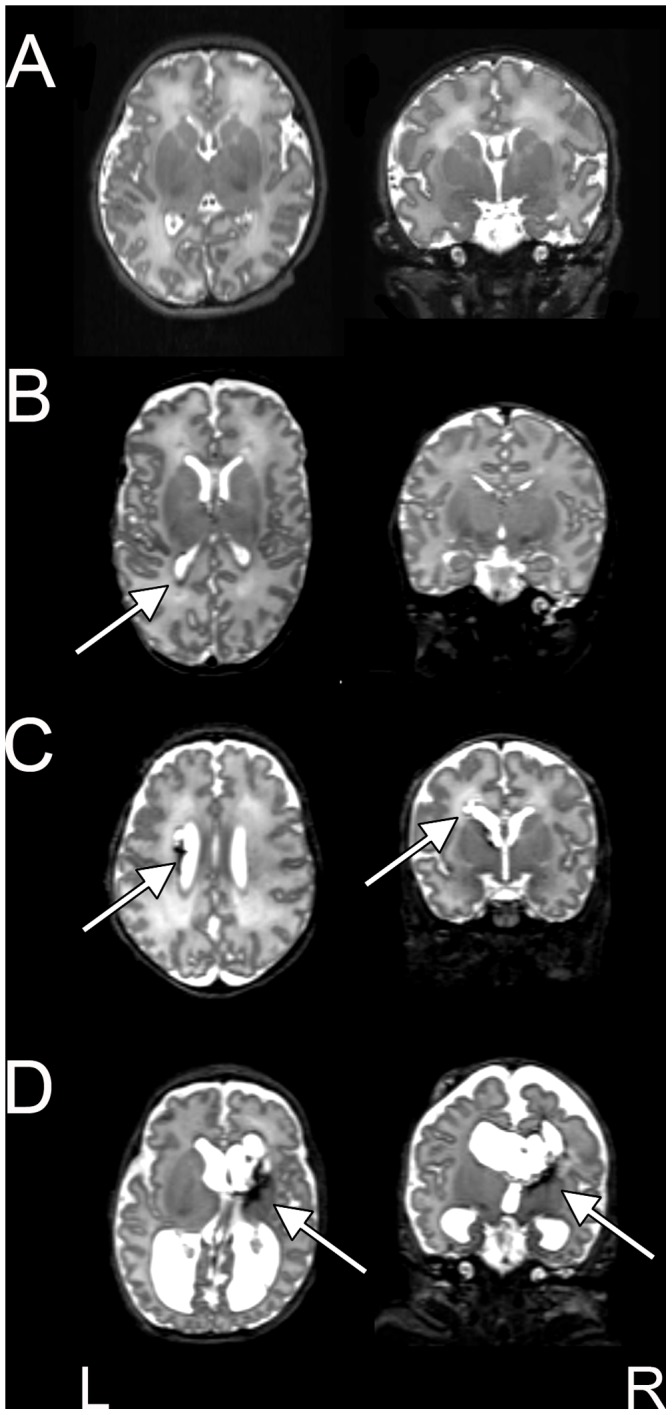
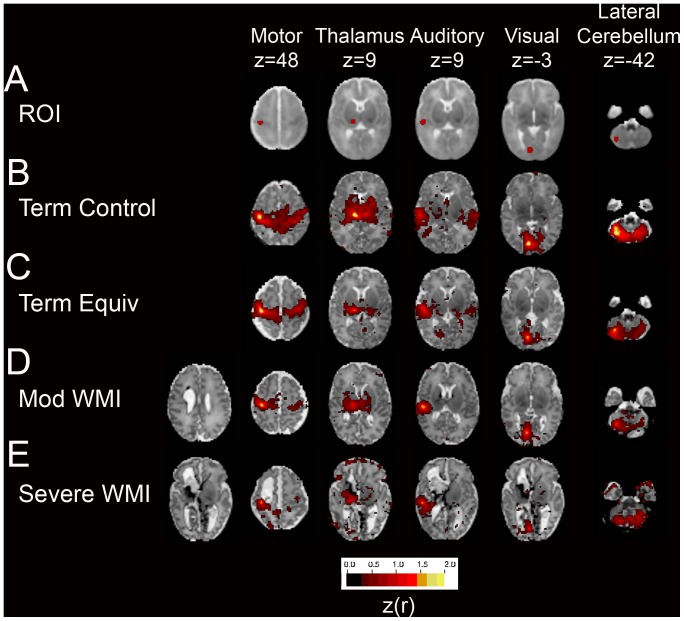
The cerebral white matter is vulnerable to injury in very preterm infants (born prior to 30 weeks gestation), resulting in a spectrum of lesions. These range from severe forms, including cystic periventricular leukomalacia and periventricular hemorrhagic infarction, to minor focal punctate lesions. Moderate to severe white matter injury in preterm infants has been shown to predict later neurodevelopmental disability, although outcomes can vary widely in infants with qualitatively comparable lesions. Resting state functional connectivity magnetic resonance imaging has been increasingly utilized in neurodevelopmental investigations and may provide complementary information regarding the impact of white matter injury on the developing brain. We performed resting state functional connectivity magnetic resonance imaging at term equivalent postmenstrual age in fourteen preterm infants with moderate to severe white matter injury secondary to periventricular hemorrhagic infarction. In these subjects, resting state networks were identifiable throughout the brain. Patterns of aberrant functional connectivity were observed and depended upon injury severity. Comparisons were performed against data obtained from prematurely-born infants with mild white matter injury and healthy, term-born infants and demonstrated group differences. These results reveal structural-functional correlates of preterm white matter injury and carry implications for future investigations of neurodevelopmental disability.
Conflict of interest statement
Figures




References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
