

Estimation of HIV incidence in a large, community-based, randomized clinical trial: NIMH project accept (HIV Prevention Trials Network 043)
- PMID: 23874597
- PMCID: PMC3708944
- DOI: 10.1371/journal.pone.0068349
Estimation of HIV incidence in a large, community-based, randomized clinical trial: NIMH project accept (HIV Prevention Trials Network 043)
Abstract
Background: National Institute of Mental Health Project Accept (HIV Prevention Trials Network [HPTN] 043) is a large, Phase III, community-randomized, HIV prevention trial conducted in 48 matched communities in Africa and Thailand. The study intervention included enhanced community-based voluntary counseling and testing. The primary endpoint was HIV incidence, assessed in a single, cross-sectional, post-intervention survey of >50,000 participants.
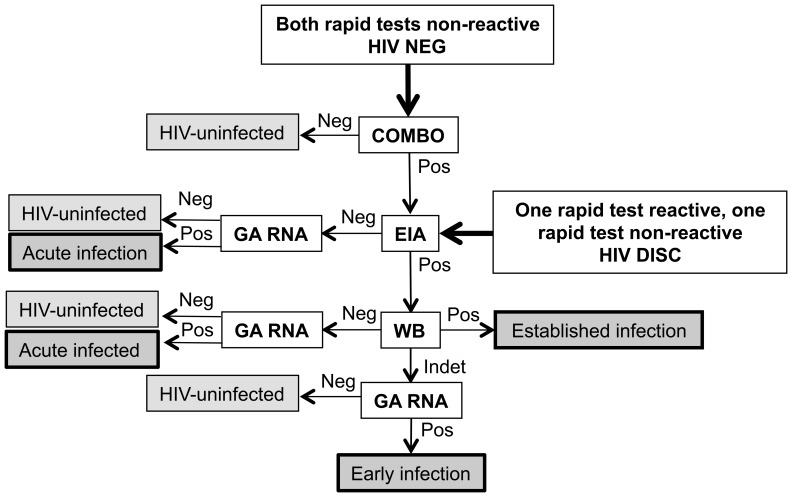
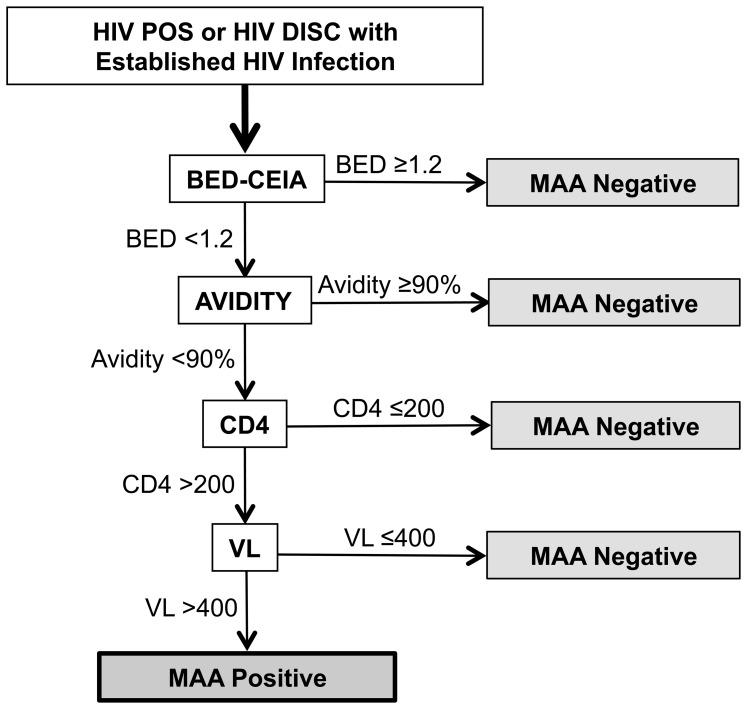
Methods: HIV rapid tests were performed in-country. HIV status was confirmed at a central laboratory in the United States. HIV incidence was estimated using a multi-assay algorithm (MAA) that included the BED capture immunoassay, an avidity assay, CD4 cell count, and HIV viral load.
Results: Data from Thailand was not used in the endpoint analysis because HIV prevalence was low. Overall, 7,361 HIV infections were identified (4 acute, 3 early, and 7,354 established infections). Samples from established infections were analyzed using the MAA; 467 MAA positive samples were identified; 29 of those samples were excluded because they contained antiretroviral drugs. HIV prevalence was 16.5% (range at study sites: 5.93% to 30.8%). HIV incidence was 1.60% (range at study sites: 0.78% to 3.90%).
Conclusions: In this community-randomized trial, a MAA was used to estimate HIV incidence in a single, cross-sectional post-intervention survey. Results from this analysis were subsequently used to compare HIV incidence in the control and intervention communities.
Trial registration: ClinicalTrials.gov NCT00203749.
Conflict of interest statement
Figures

References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- U01-AI068617/AI/NIAID NIH HHS/United States
- U01 MH066701/MH/NIMH NIH HHS/United States
- U01 MH066687/MH/NIMH NIH HHS/United States
- UM1-AI068619/AI/NIAID NIH HHS/United States
- U01-MH066701/MH/NIMH NIH HHS/United States
- R01 AI095068/AI/NIAID NIH HHS/United States
- U01-AI068619/AI/NIAID NIH HHS/United States
- R01-AI095068/AI/NIAID NIH HHS/United States
- U01 MH066688/MH/NIMH NIH HHS/United States
- U01-MH066702/MH/NIMH NIH HHS/United States
- UM1 AI069399/AI/NIAID NIH HHS/United States
- ImNIH/Intramural NIH HHS/United States
- U01MH066687/MH/NIMH NIH HHS/United States
- UM1 AI068619/AI/NIAID NIH HHS/United States
- UM1 AI068613/AI/NIAID NIH HHS/United States
- U01 MH066702/MH/NIMH NIH HHS/United States
- UM1-AI068613/AI/NIAID NIH HHS/United States
- U01-AI068613/AI/NIAID NIH HHS/United States
- U01-MH066688/MH/NIMH NIH HHS/United States
- UM1-AI068617/AI/NIAID NIH HHS/United States
- UM1 AI068617/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
