

Interplay between immune responses to HLA and non-HLA self-antigens in allograft rejection
- PMID: 23876679
- PMCID: PMC3813452
- DOI: 10.1016/j.humimm.2013.07.002
Interplay between immune responses to HLA and non-HLA self-antigens in allograft rejection
Abstract
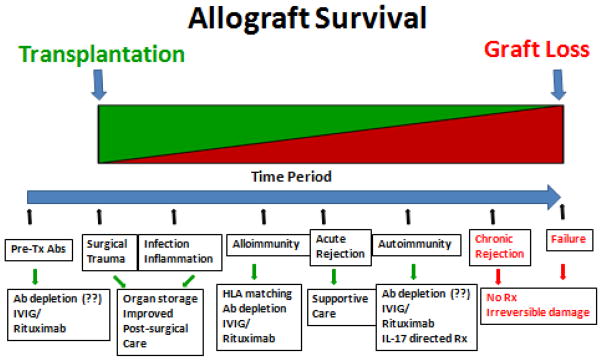
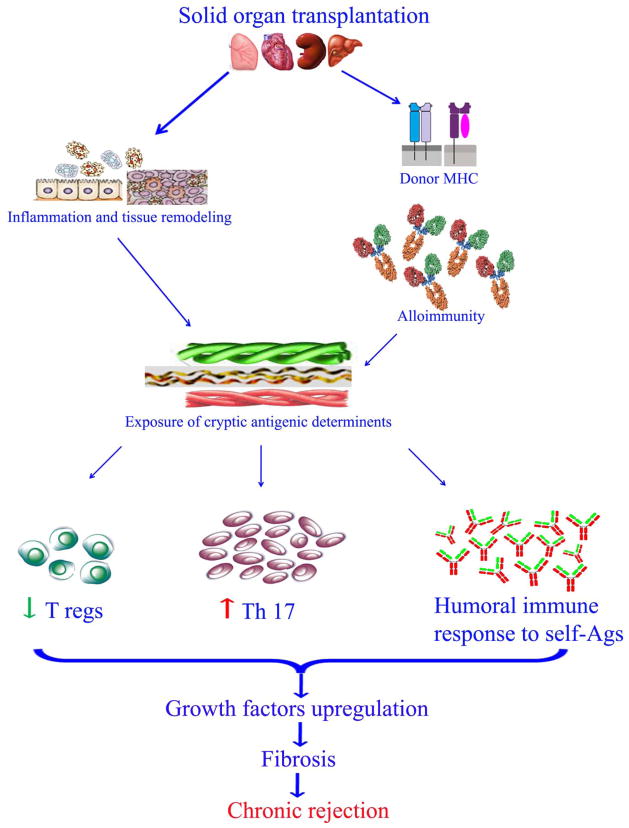
Recent studies strongly suggest an increasing role for immune responses against self-antigens (Ags) which are not encoded by the major histocompatibility complex in the immunopathogenesis of allograft rejection. Although, improved surgical techniques coupled with improved methods to detect and avoid sensitization against donor human leukocyte antigen (HLA) have improved the immediate and short term function of transplanted organs. However, acute and chronic rejection still remains a vexing problem for the long term function of the transplanted organ. Immediately following organ transplantation, several factors both immune and non immune mechanisms lead to the development of local inflammatory milieu which sets the stage for allograft rejection. Traditionally, development of antibodies (Abs) against mismatched donor HLA have been implicated in the development of Ab mediated rejection. However, recent studies from our laboratory and others have demonstrated that development of humoral and cellular immune responses against non-HLA self-Ags may contribute in the pathogenesis of allograft rejection. There are reports demonstrating that immune responses to self-Ags especially Abs to the self-Ags as well as cellular immune responses especially through IL17 has significant pro-fibrotic properties leading to chronic allograft failure. This review summarizes recent studies demonstrating the role for immune responses to self-Ags in allograft immunity leading to rejection as well as present recent evidence suggesting there is interplay between allo- and autoimmunity leading to allograft dysfunction.
Keywords: AEC; AGTR1; AMR; APC; Ab; Ag; BOS; CAN; CAV; CMV; CR; ColV; DC; DSA; HCV; HIF-1α; HLA; IRI; Kα1 tubulin; Kα1T; MHC; MHC class I related chain A; MICA; NHBE; OAD; OLT; PGD; TG; TRALI; Tx; airway epithelial cells; angiotensin II type 1 receptor; antibody; antibody mediated rejection; antigen; antigen presenting cell; bronchiolitis obliterans syndrome; cardiac allograft vasculopathy; chronic allograft nephropathy; chronic rejection; collagen V; cytomegalovirus; dendritic cells; donor specific antibodies; hepatitis C virus; human bronchial epithelial; human leukocyte antigen; hypoxia inducible factor; iNKT; invariant natural killer T cells; mTOR; major histocompatibility complex; mammalian target of rapamycin; obliterative airway disease; orthotopic liver transplantation; primary graft dysfunction; schemia/reperfusion injury; transfusion-related lung injury; transplant glomerulopathy; transplantation.
Copyright © 2013 American Society for Histocompatibility and Immunogenetics. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
None of the authors have any conflicts of interest to disclose.
Figures
References
-
- Game DS, Lechler RI. Pathways of allorecognition: implications for transplantation tolerance. Transpl Immunol. 2002;10(2–3):101. - PubMed
-
- Hernandez-Fuentes MP, Baker RJ, Lechler RI. The alloresponse. Rev Immunogenet. 1999;1(3):282. - PubMed
-
- Herrera OB, Golshayan D, Tibbott R, Salcido Ochoa F, James MJ, Marelli-Berg FM, Lechler RI. A novel pathway of alloantigen presentation by dendritic cells. J Immunol. 2004;173(8):4828. - PubMed
-
- Pimenta-Araujo R, Mascarell L, Huesca M, Cumano A, Bandeira A. Embryonic thymic epithelium naturally devoid of APCs is acutely rejected in the absence of indirect recognition. J Immunol. 2001;167(9):5034. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
