

Corneal nerve loss detected with corneal confocal microscopy is symmetrical and related to the severity of diabetic polyneuropathy
- PMID: 23877983
- PMCID: PMC3816900
- DOI: 10.2337/dc13-0193
Corneal nerve loss detected with corneal confocal microscopy is symmetrical and related to the severity of diabetic polyneuropathy
Abstract
Objective: To establish if corneal nerve loss, detected using in vivo corneal confocal microscopy (IVCCM), is symmetrical between right and left eyes and relates to the severity of diabetic neuropathy.
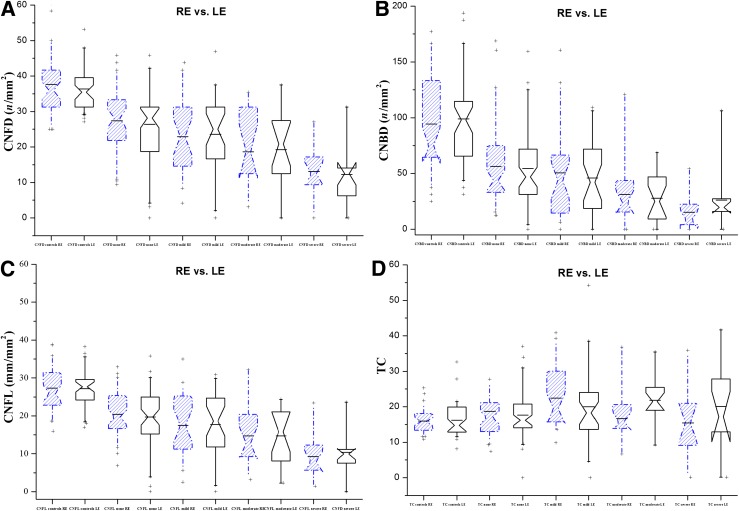
Research design and methods: Patients (n = 111) with type 1 and type 2 diabetes and 47 age-matched healthy control subjects underwent detailed assessment and stratification into no (n = 50), mild (n = 26), moderate (n = 17), and severe (n = 18) neuropathy. IVCCM was performed in both eyes and corneal nerve fiber density (CNFD), branch density (CNBD), and fiber length (CNFL) and the tortuosity coefficient were quantified.
Results: All corneal nerve parameters differed significantly between diabetic patients and control subjects and progressively worsened with increasing severity of neuropathy. The reduction in CNFD, CNBD, and CNFL was symmetrical in all groups except in patients with severe neuropathy.
Conclusions: IVCCM noninvasively detects corneal nerve loss, which relates to the severity of neuropathy, and is symmetrical, except in those with severe diabetic neuropathy.
Figures
References
-
- Dyck PJ, Giannini C. Pathologic alterations in the diabetic neuropathies of humans: a review. J Neuropathol Exp Neurol 1996;55:1181–1193 - PubMed
-
- Boulton AJ, Vileikyte L, Ragnarson-Tennvall G, Apelqvist J. The global burden of diabetic foot disease. Lancet 2005;366:1719–1724 - PubMed
-
- Boulton AJ, Malik RA, Arezzo JC, Sosenko JM. Diabetic somatic neuropathies. Diabetes Care 2004;27:1458–1486 - PubMed
-
- Quattrini C, Tavakoli M, Jeziorska M, et al. Surrogate markers of small fiber damage in human diabetic neuropathy. Diabetes 2007;56:2148–2154 - PubMed
-
- Løseth S, Stålberg E, Jorde R, Mellgren SI. Early diabetic neuropathy: thermal thresholds and intraepidermal nerve fibre density in patients with normal nerve conduction studies. J Neurol 2008;255:1197–1202 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
