

Cortical spreading depression as a target for anti-migraine agents
- PMID: 23879550
- PMCID: PMC3728002
- DOI: 10.1186/1129-2377-14-62
Cortical spreading depression as a target for anti-migraine agents
Abstract
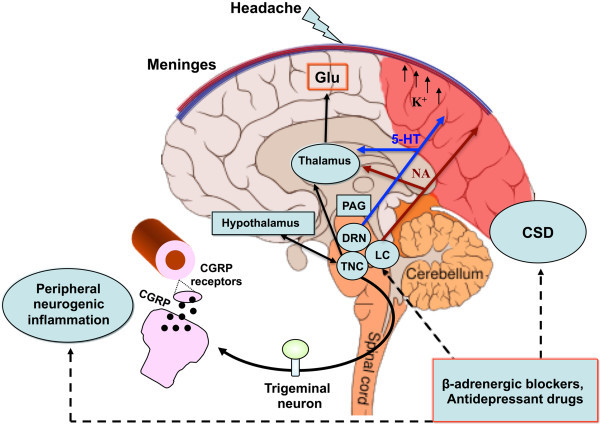
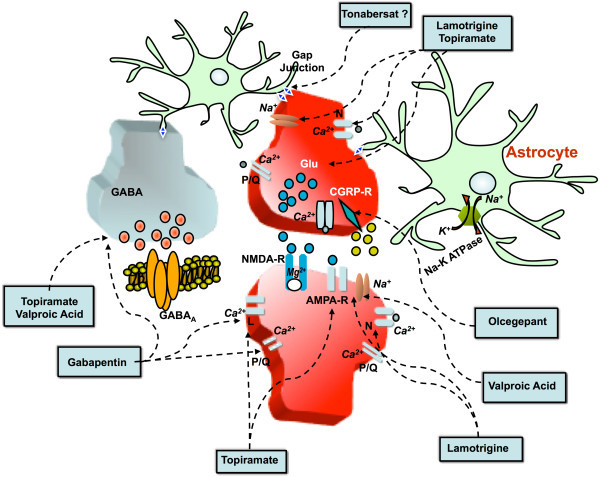
Spreading depression (SD) is a slowly propagating wave of neuronal and glial depolarization lasting a few minutes, that can develop within the cerebral cortex or other brain areas after electrical, mechanical or chemical depolarizing stimulations. Cortical SD (CSD) is considered the neurophysiological correlate of migraine aura. It is characterized by massive increases in both extracellular K⁺ and glutamate, as well as rises in intracellular Na⁺ and Ca²⁺. These ionic shifts produce slow direct current (DC) potential shifts that can be recorded extracellularly. Moreover, CSD is associated with changes in cortical parenchymal blood flow. CSD has been shown to be a common therapeutic target for currently prescribed migraine prophylactic drugs. Yet, no effects have been observed for the antiepileptic drugs carbamazepine and oxcarbazepine, consistent with their lack of efficacy on migraine. Some molecules of interest for migraine have been tested for their effect on CSD. Specifically, blocking CSD may play an enabling role for novel benzopyran derivative tonabersat in preventing migraine with aura. Additionally, calcitonin gene-related peptide (CGRP) antagonists have been recently reported to inhibit CSD, suggesting the contribution of CGRP receptor activation to the initiation and maintenance of CSD not only at the classic vascular sites, but also at a central neuronal level. Understanding what may be lying behind this contribution, would add further insights into the mechanisms of actions for "gepants", which may be pivotal for the effectiveness of these drugs as anti-migraine agents. CSD models are useful tools for testing current and novel prophylactic drugs, providing knowledge on mechanisms of action relevant for migraine.
Figures
References
-
- Lauritzen M, Dreier JP, Fabricius M, Hartings JA, Graf R, Strong AJ. Clinical relevance of cortical spreading depression in neurological disorders: migraine, malignant stroke, subarachnoid and intracranial hemorrhage, and traumatic brain injury. J Cereb Blood Flow Metab. 2011;14:17–35. doi: 10.1038/jcbfm.2010.191. - DOI - PMC - PubMed
-
- Somjen GG. Mechanisms of spreading depression and hypoxic spreading depression-like depolarization. Physiol Rev. 2001;14:1065–1096. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
