

Comparative assessment of absolute cardiovascular disease risk characterization from non-laboratory-based risk assessment in South African populations
- PMID: 23880010
- PMCID: PMC3734109
- DOI: 10.1186/1741-7015-11-170
Comparative assessment of absolute cardiovascular disease risk characterization from non-laboratory-based risk assessment in South African populations
Abstract
Background: All rigorous primary cardiovascular disease (CVD) prevention guidelines recommend absolute CVD risk scores to identify high- and low-risk patients, but laboratory testing can be impractical in low- and middle-income countries. The purpose of this study was to compare the ranking performance of a simple, non-laboratory-based risk score to laboratory-based scores in various South African populations.
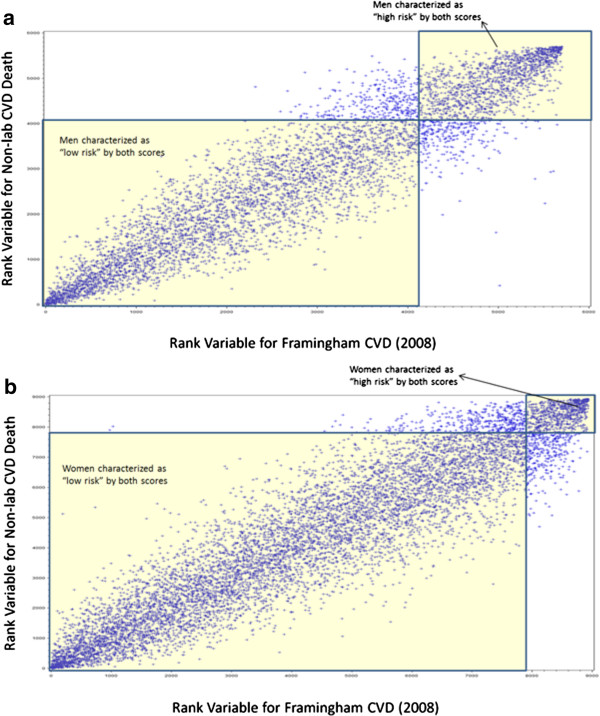
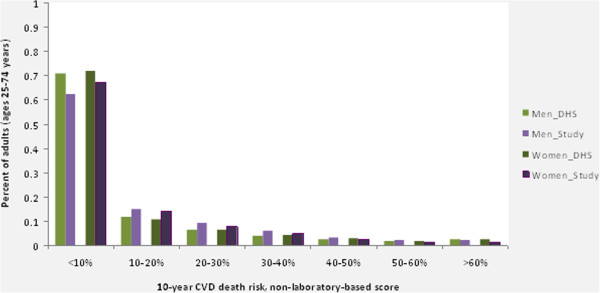
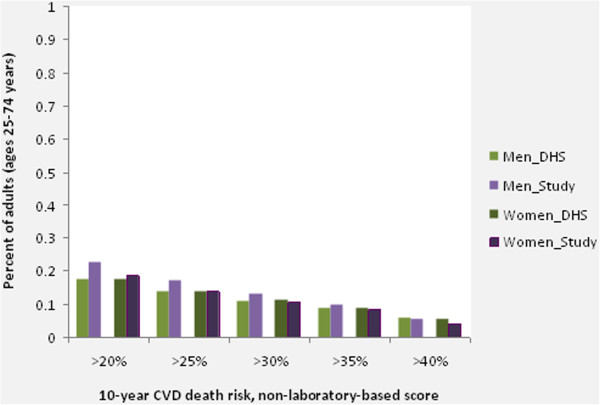
Methods: We calculated and compared 10-year CVD (or coronary heart disease (CHD)) risk for 14,772 adults from thirteen cross-sectional South African populations (data collected from 1987 to 2009). Risk characterization performance for the non-laboratory-based score was assessed by comparing rankings of risk with six laboratory-based scores (three versions of Framingham risk, SCORE for high- and low-risk countries, and CUORE) using Spearman rank correlation and percent of population equivalently characterized as 'high' or 'low' risk. Total 10-year non-laboratory-based risk of CVD death was also calculated for a representative cross-section from the 1998 South African Demographic Health Survey (DHS, n = 9,379) to estimate the national burden of CVD mortality risk.
Results: Spearman correlation coefficients for the non-laboratory-based score with the laboratory-based scores ranged from 0.88 to 0.986. Using conventional thresholds for CVD risk (10% to 20% 10-year CVD risk), 90% to 92% of men and 94% to 97% of women were equivalently characterized as 'high' or 'low' risk using the non-laboratory-based and Framingham (2008) CVD risk score. These results were robust across the six risk scores evaluated and the thirteen cross-sectional datasets, with few exceptions (lower agreement between the non-laboratory-based and Framingham (1991) CHD risk scores). Approximately 18% of adults in the DHS population were characterized as 'high CVD risk' (10-year CVD death risk >20%) using the non-laboratory-based score.
Conclusions: We found a high level of correlation between a simple, non-laboratory-based CVD risk score and commonly-used laboratory-based risk scores. The burden of CVD mortality risk was high for men and women in South Africa. The policy and clinical implications are that fast, low-cost screening tools can lead to similar risk assessment results compared to time- and resource-intensive approaches. Until setting-specific cohort studies can derive and validate country-specific risk scores, non-laboratory-based CVD risk assessment could be an effective and efficient primary CVD screening approach in South Africa.
Figures
Similar articles
-
Comparison of Nonblood-Based and Blood-Based Total CV Risk Scores in Global Populations.Glob Heart. 2016 Mar;11(1):37-46.e2. doi: 10.1016/j.gheart.2015.12.003. Glob Heart. 2016. PMID: 27102021
-
A comparative assessment of non-laboratory-based versus commonly used laboratory-based cardiovascular disease risk scores in the NHANES III population.PLoS One. 2011;6(5):e20416. doi: 10.1371/journal.pone.0020416. Epub 2011 May 31. PLoS One. 2011. PMID: 21655241 Free PMC article.
-
Cardiovascular disease risk prediction in sub-Saharan African populations - Comparative analysis of risk algorithms in the RODAM study.Int J Cardiol. 2018 Mar 1;254:310-315. doi: 10.1016/j.ijcard.2017.11.082. Epub 2018 Jan 28. Int J Cardiol. 2018. PMID: 29407113
-
Evaluation of the performance of existing non-laboratory based cardiovascular risk assessment algorithms.BMC Cardiovasc Disord. 2013 Dec 28;13:123. doi: 10.1186/1471-2261-13-123. BMC Cardiovasc Disord. 2013. PMID: 24373202 Free PMC article. Review.
-
Performance of the Framingham risk models and pooled cohort equations for predicting 10-year risk of cardiovascular disease: a systematic review and meta-analysis.BMC Med. 2019 Jun 13;17(1):109. doi: 10.1186/s12916-019-1340-7. BMC Med. 2019. PMID: 31189462 Free PMC article.
Cited by
-
Quality Improvement for Cardiovascular Disease Care in Low- and Middle-Income Countries: A Systematic Review.PLoS One. 2016 Jun 14;11(6):e0157036. doi: 10.1371/journal.pone.0157036. eCollection 2016. PLoS One. 2016. PMID: 27299563 Free PMC article.
-
Association of predicted 10 years cardiovascular mortality risk with duration of HIV infection and antiretroviral therapy among HIV-infected individuals in Durban, South Africa.Diabetol Metab Syndr. 2019 Dec 16;11:105. doi: 10.1186/s13098-019-0502-2. eCollection 2019. Diabetol Metab Syndr. 2019. PMID: 31890039 Free PMC article.
-
Prognostic validation of a non-laboratory and a laboratory based cardiovascular disease risk score in multiple regions of the world.Heart. 2018 Apr;104(7):581-587. doi: 10.1136/heartjnl-2017-311609. Epub 2017 Oct 24. Heart. 2018. PMID: 29066611 Free PMC article.
-
Prevalence of Pragmatically Defined High CV Risk and its Correlates in LMIC: A Report From 10 LMIC Areas in Africa, Asia, and South America.Glob Heart. 2016 Mar;11(1):27-36. doi: 10.1016/j.gheart.2015.12.004. Glob Heart. 2016. PMID: 27102020 Free PMC article.
-
An assessment of community health workers' ability to screen for cardiovascular disease risk with a simple, non-invasive risk assessment instrument in Bangladesh, Guatemala, Mexico, and South Africa: an observational study.Lancet Glob Health. 2015 Sep;3(9):e556-63. doi: 10.1016/S2214-109X(15)00143-6. Epub 2015 Jul 14. Lancet Glob Health. 2015. PMID: 26187361 Free PMC article.
References
-
- Jackson R, Lawes CM, Bennett DA, Milne RJ, Rodgers A. Treatment with drugs to lower blood pressure and blood cholesterol based on an individual’s absolute cardiovascular risk. Lancet. 2005;365:434–441. - PubMed
-
- Conroy RM, Pyorala K, Fitzgerald AP, Sans S, Menotti A, De Backer G, De Bacquer D, Ducimetiere P, Jousilahti P, Keil U, Njølstad I, Oganov RG, Thomsen T, Tunstall-Pedoe H, Tverdal A, Wedel H, Whincup P, Wilhelmsen L, Graham IM. SCORE project group. Estimation of ten-year risk of fatal cardiovascular disease in Europe: the SCORE project. Eur Heart J. 2003;24:987–1003. doi: 10.1016/S0195-668X(03)00114-3. - DOI - PubMed
-
- Evans A, Salomaa V, Kulathinal S, Asplund K, Cambien F, Ferrario M, Perola M, Peltonen L, Shields D, Tunstall-Pedoe H, Kuulasmaa K. MORGAM Project. MORGAM (an international pooling of cardiovascular cohorts) Int J Epidemiol. 2005;34:21–27. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
