

Tolerance develops to the antiallodynic effects of the peripherally acting opioid loperamide hydrochloride in nerve-injured rats
- PMID: 23880055
- PMCID: PMC3863910
- DOI: 10.1016/j.pain.2013.07.023
Tolerance develops to the antiallodynic effects of the peripherally acting opioid loperamide hydrochloride in nerve-injured rats
Abstract
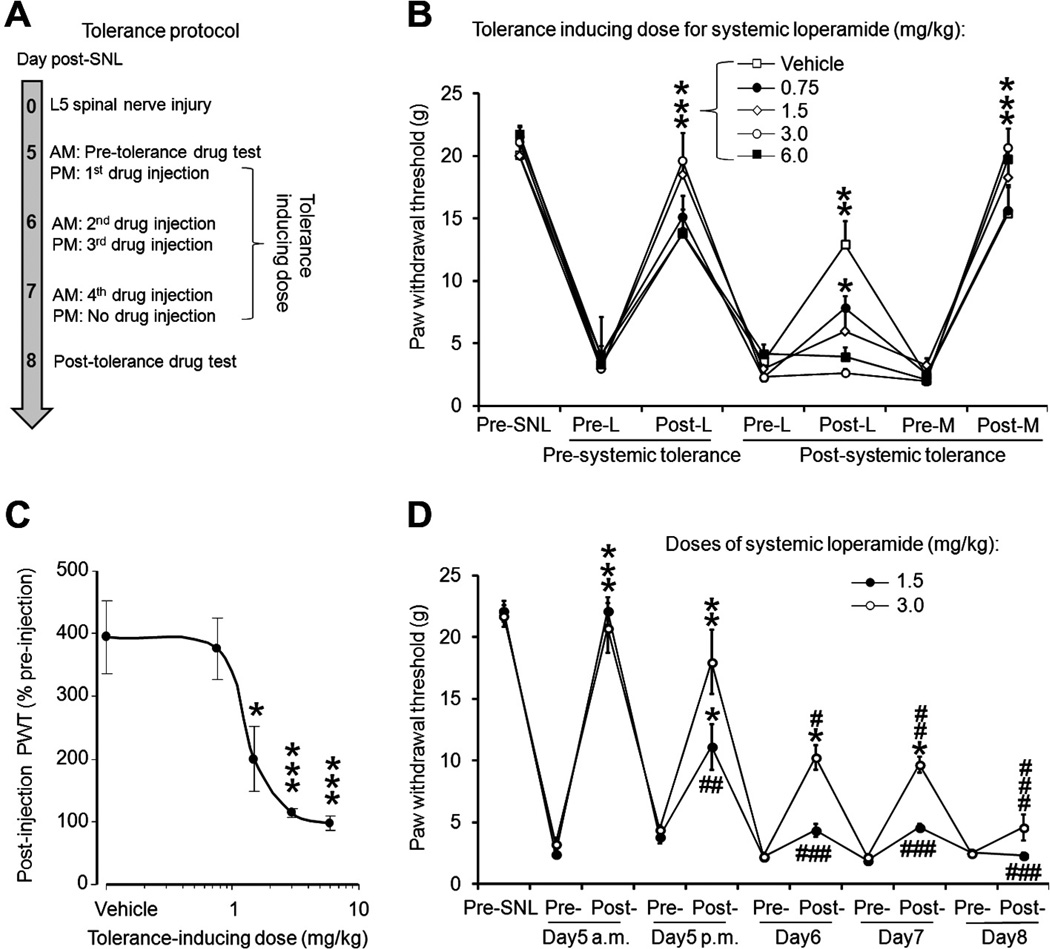
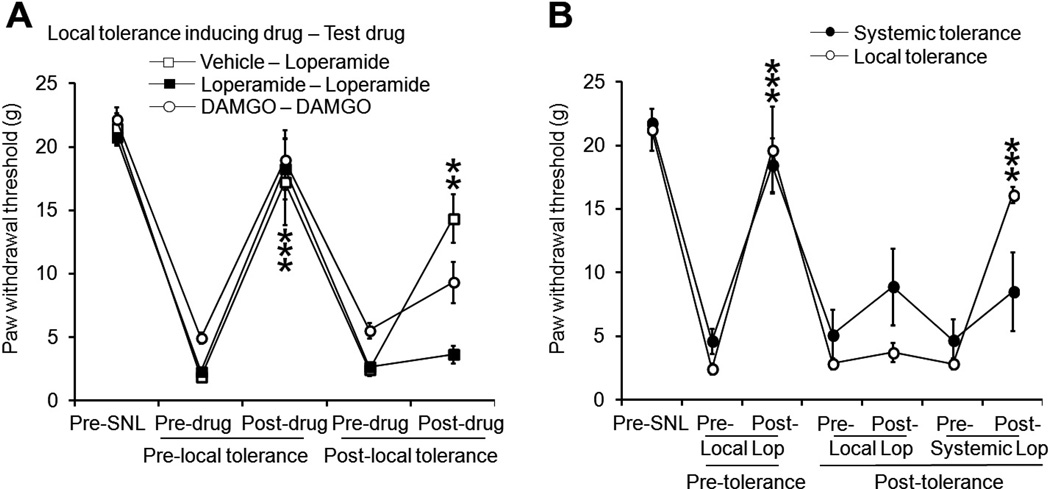
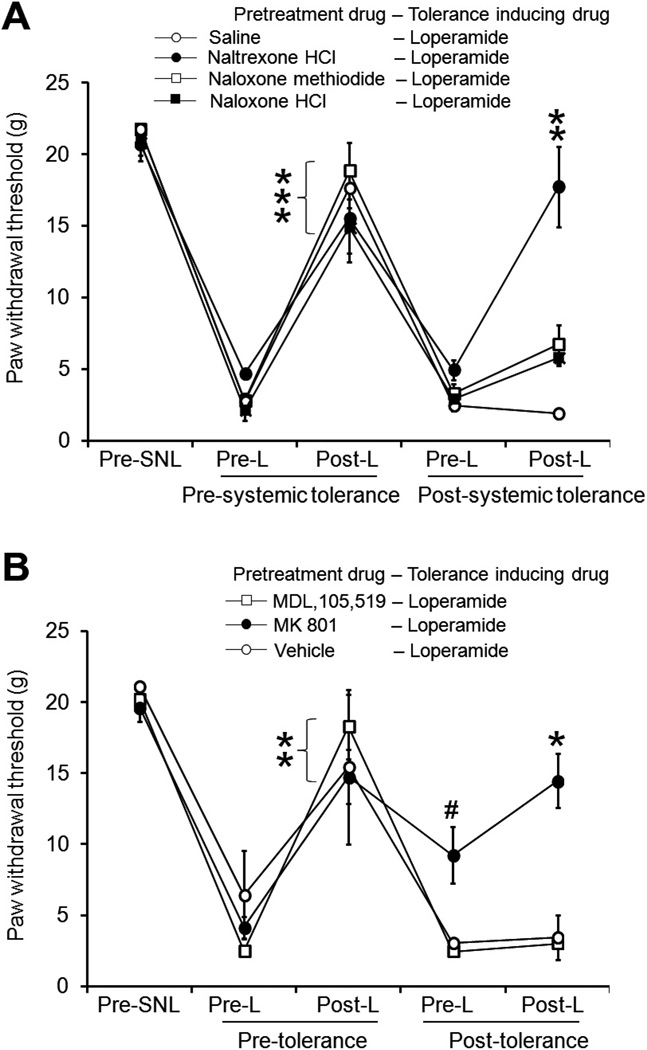
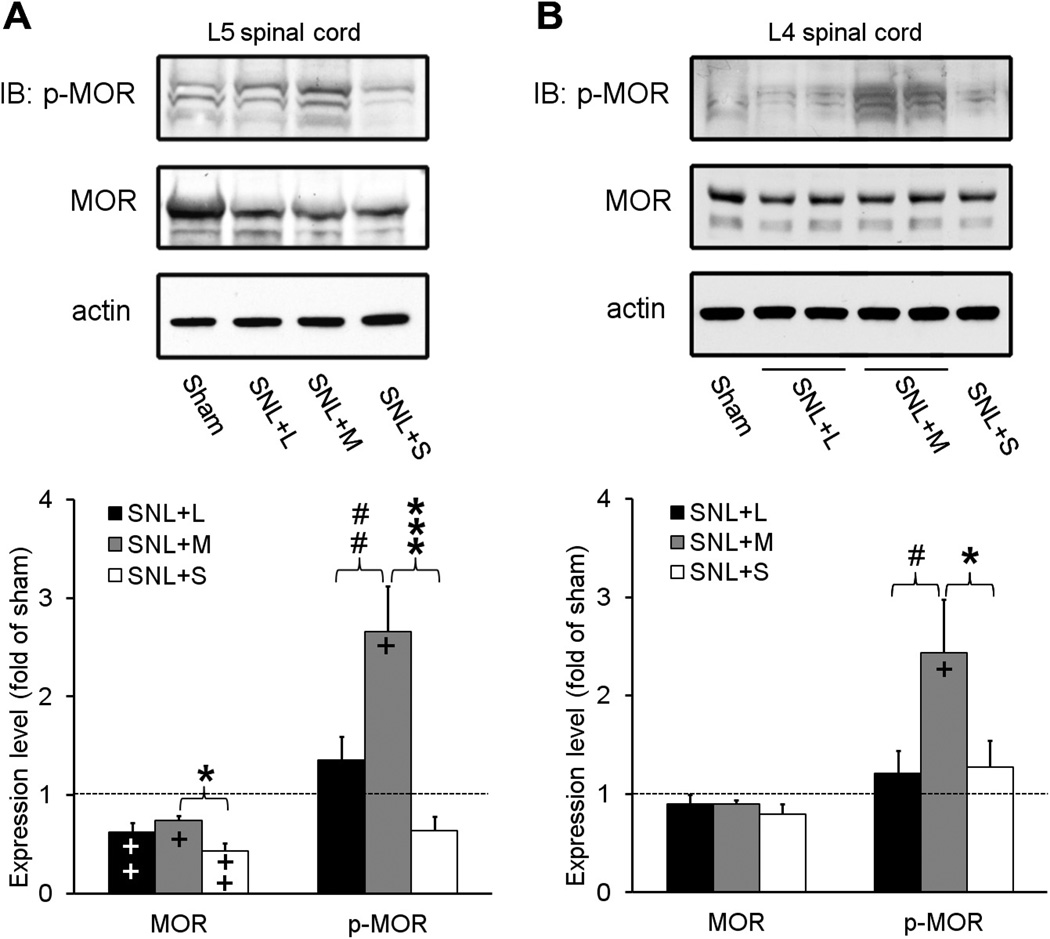
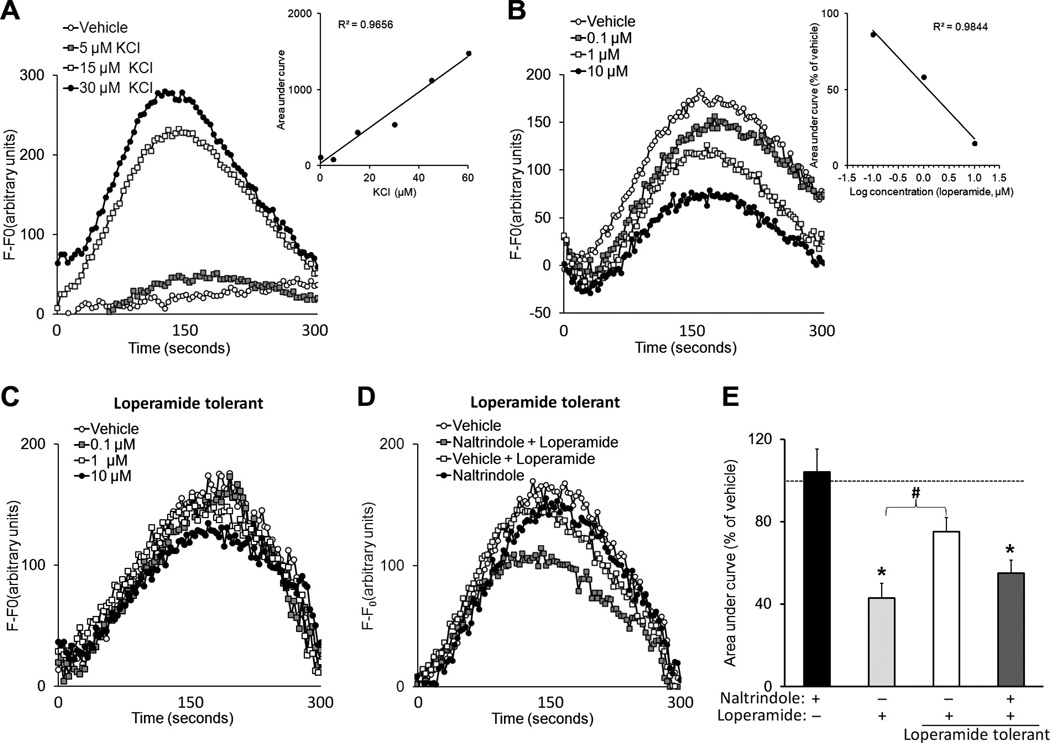
Peripherally acting opioids are potentially attractive drugs for the clinical management of certain chronic pain states due to the lack of centrally mediated adverse effects. However, it remains unclear whether tolerance develops to peripheral opioid analgesic effects under neuropathic pain conditions. We subjected rats to L5 spinal nerve ligation (SNL) and examined the analgesic effects of repetitive systemic and local administration of loperamide hydrochloride, a peripherally acting opioid agonist. We found that the inhibition of mechanical hypersensitivity, an important manifestation of neuropathic pain, by systemic loperamide (1.5mg/kg subcutaneously) decreased after repetitive drug treatment (tolerance-inducing dose: 0.75 to 6.0mg/kg subcutaneously). Similarly, repeated intraplantar injection of loperamide (150 μg/50 μL intraplantarly) and D-Ala(2)-MePhe(4)-Glyol(5) enkephalin (300 μg/50 μL), a highly selective mu-opioid receptor (MOR) agonist, also resulted in decreased inhibition of mechanical hypersensitivity. Pretreatment with naltrexone hydrochloride (5mg/kg intraperitoneally) and MK-801 (0.2mg/kg intraperitoneally) attenuated systemic loperamide tolerance. Western blot analysis showed that repetitive systemic administration of morphine (3mg/kg subcutaneously), but not loperamide (3mg/kg subcutaneously) or saline, significantly increased MOR phosphorylation in the spinal cord of SNL rats. In cultured rat dorsal root ganglion neurons, loperamide dose-dependently inhibited KCl-induced increases in [Ca(2+)]i. However, this drug effect significantly decreased in cells pretreated with loperamide (3 μM, 72 hours). Intriguingly, in loperamide-tolerant cells, the delta-opioid receptor antagonist naltrindole restored loperamide's inhibition of KCl-elicited [Ca(2+)]i increase. Our findings indicate that animals with neuropathic pain may develop acute tolerance to the antiallodynic effects of peripherally acting opioids after repetitive systemic and local drug administration.
Keywords: Nerve injury; Neuropathic pain; Peripheral opioid receptor; Rats; Tolerance.
Copyright © 2013 International Association for the Study of Pain. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Abdelhamid EE, Sultana M, Portoghese PS, Takemori AE. Selective blockage of delta opioid receptors prevents the development of morphine tolerance and dependence in mice. J Pharmacol Exp Ther. 1991;258:299–303. - PubMed
-
- Bailey CP, Smith FL, Kelly E, Dewey WL, Henderson G. How important is protein kinase C in mu-opioid receptor desensitization and morphine tolerance? Trends Pharmacol Sci. 2006;27:558–565. - PubMed
-
- Baker DE. Loperamide: a pharmacological review. Rev Gastroenterol Disord. 2007;7:S11–S18. - PubMed
-
- Christensen D, Kayser V. The development of pain-related behaviour and opioid tolerance after neuropathy-inducing surgery and sham surgery. PAIN®. 2000;88:231–238. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
