

Use of multilocus variable number of tandem repeats analysis genotyping to determine the role of asymptomatic carriers in Clostridium difficile transmission
- PMID: 23881150
- PMCID: PMC3783061
- DOI: 10.1093/cid/cit475
Use of multilocus variable number of tandem repeats analysis genotyping to determine the role of asymptomatic carriers in Clostridium difficile transmission
Abstract
Background: Previous studies have suggested that asymptomatic carriers of toxigenic Clostridium difficile are a source of hospital-associated (HA) infections. Multilocus variable number of tandem repeats analysis (MLVA) is a highly discriminatory molecular subtyping tool that helps to determine possible transmission sources.
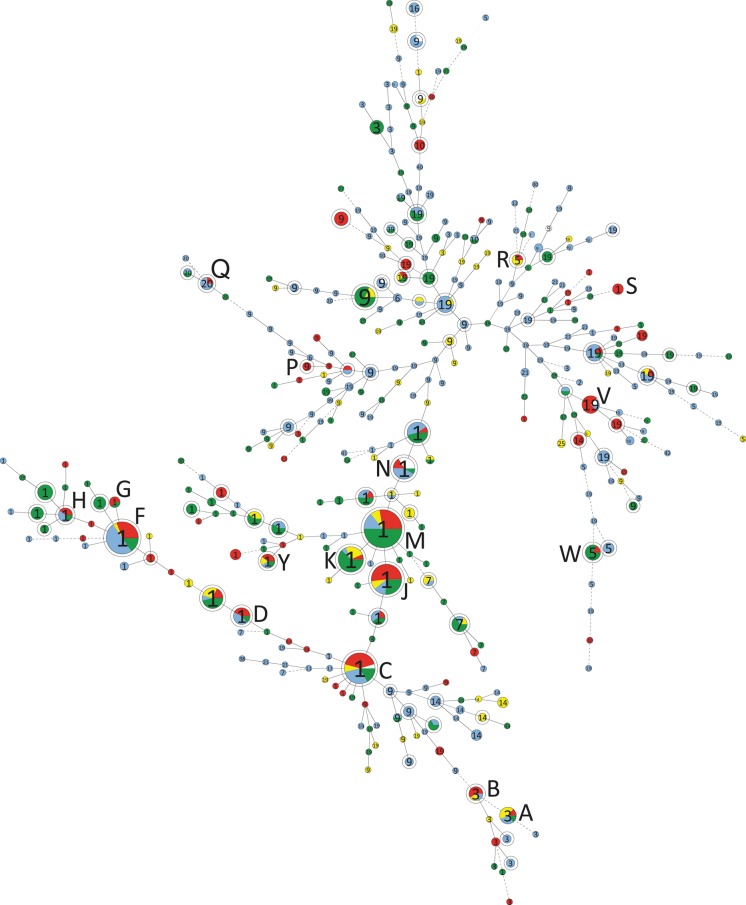
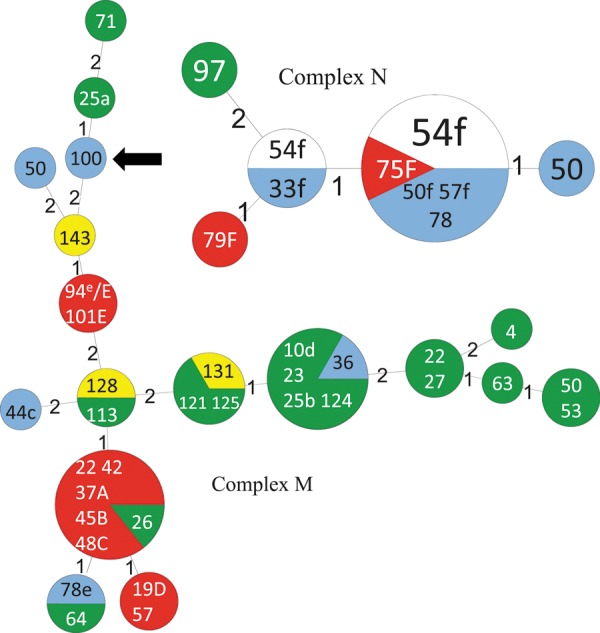
Methods: Clostridium difficile isolates were recovered from perirectal swabs collected for vancomycin-resistant Enterococcus (VRE) surveillance as well as from clinical C. difficile toxin-positive stool samples from July to November 2009 at the University of Pittsburgh Medical Center Presbyterian (UPMC). MLVA was performed to determine the genetic relationships between isolates from asymptomatic carriers and patients with HA C. difficile infection (HA-CDI). Asymptomatic carriage and HA-CDI isolates were considered to be associated if the carriage isolate was collected before the HA-CDI isolate and if the MLVA genotypes had a summed tandem-repeat difference of ≤ 2.
Results: Of 3006 patients screened, 314 (10.4%) were positive for toxigenic C. difficile, of whom 226 (7.5%) were detected only by VRE surveillance cultures. Of 56 incident cases of CDI classified as HA at UPMC during the study with available isolates, 17 (30%) cases were associated with CDI patients, whereas 16 (29%) cases were associated with carriers. Transmission events from prior bed occupants with CDI (n = 2) or carriers (n = 2) were identified in 4 of 56 cases.
Conclusions: In our hospital with an established infection control program designed to contain transmission from symptomatic CDI patients, asymptomatic carriers appear to have played an important role in transmission. Identification and isolation of carriers may be necessary to further reduce transmission of C. difficile in such settings.
Keywords: Clostridium difficile; MLVA; genotyping; screening; transmission.
Figures
Similar articles
-
Colonization of toxigenic Clostridium difficile among ICU patients: a prospective study.BMC Infect Dis. 2016 Aug 9;16:397. doi: 10.1186/s12879-016-1729-2. BMC Infect Dis. 2016. PMID: 27506470 Free PMC article.
-
Effect of Detecting and Isolating Clostridium difficile Carriers at Hospital Admission on the Incidence of C difficile Infections: A Quasi-Experimental Controlled Study.JAMA Intern Med. 2016 Jun 1;176(6):796-804. doi: 10.1001/jamainternmed.2016.0177. JAMA Intern Med. 2016. PMID: 27111806
-
Whole genome sequencing of toxigenic Clostridium difficile in asymptomatic carriers: insights into possible role in transmission.J Hosp Infect. 2019 Jun;102(2):125-134. doi: 10.1016/j.jhin.2018.10.012. Epub 2018 Oct 22. J Hosp Infect. 2019. PMID: 30359648
-
Diverse Sources and Latent Reservoirs of Community-Associated Clostridioides difficile Infection.Clin Infect Dis. 2025 Feb 5;80(1):37-42. doi: 10.1093/cid/ciae429. Clin Infect Dis. 2025. PMID: 39215602 Review.
-
Clostridium difficile and One Health.Clin Microbiol Infect. 2020 Jul;26(7):857-863. doi: 10.1016/j.cmi.2019.10.023. Epub 2019 Nov 1. Clin Microbiol Infect. 2020. PMID: 31682985 Review.
Cited by
-
Isolation of C. difficile Carriers Alone and as Part of a Bundle Approach for the Prevention of Clostridium difficile Infection (CDI): A Mathematical Model Based on Clinical Study Data.PLoS One. 2016 Jun 3;11(6):e0156577. doi: 10.1371/journal.pone.0156577. eCollection 2016. PLoS One. 2016. PMID: 27258068 Free PMC article.
-
Unlocking the Sporicidal Potential of Ethanol: Induced Sporicidal Activity of Ethanol against Clostridium difficile and Bacillus Spores under Altered Physical and Chemical Conditions.PLoS One. 2015 Jul 15;10(7):e0132805. doi: 10.1371/journal.pone.0132805. eCollection 2015. PLoS One. 2015. PMID: 26177038 Free PMC article.
-
Comparative Genomics of Clostridioides difficile.Adv Exp Med Biol. 2024;1435:199-218. doi: 10.1007/978-3-031-42108-2_10. Adv Exp Med Biol. 2024. PMID: 38175477
-
Environmental transmission of Clostridioides difficile ribotype 027 at a long-term care facility; an outbreak investigation guided by whole genome sequencing.Infect Control Hosp Epidemiol. 2018 Nov;39(11):1322-1329. doi: 10.1017/ice.2018.230. Epub 2018 Sep 26. Infect Control Hosp Epidemiol. 2018. PMID: 30253813 Free PMC article.
-
Core genome multilocus sequence typing of Clostridioides difficile to investigate transmission in the hospital setting.Eur J Clin Microbiol Infect Dis. 2023 Dec;42(12):1469-1476. doi: 10.1007/s10096-023-04676-9. Epub 2023 Oct 23. Eur J Clin Microbiol Infect Dis. 2023. PMID: 37870711 Free PMC article.
References
-
- Clabots CR, Johnson S, Olson MM, Peterson LR, Gerding DN. Acquisition of Clostridium difficile by hospitalized patients: evidence for colonized new admissions as a source of infection. J Infect Dis. 1992;166:561–7. - PubMed
-
- Johnson S, Clabots CR, Linn FV, Olson MM, Peterson LR, Gerding DN. Nosocomial Clostridium difficile colonisation and disease. Lancet. 1990;336:97–100. - PubMed
-
- McFarland LV, Mulligan ME, Kwok RY, Stamm WE. Nosocomial acquisition of Clostridium difficile infection. N Engl J Med. 1989;320:204–10. - PubMed
-
- Samore MH, DeGirolami PC, Tlucko A, Lichtenberg DA, Melvin ZA, Karchmer AW. Clostridium difficile colonization and diarrhea at a tertiary care hospital. Clin Infect Dis. 1994;18:181–7. - PubMed
-
- Shim JK, Johnson S, Samore MH, Bliss DZ, Gerding DN. Primary symptomless colonisation by Clostridium difficile and decreased risk of subsequent diarrhoea. Lancet. 1998;351:633–6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
