

Is DOPA-Responsive Hypokinesia Responsible for Bimanual Coordination Deficits in Parkinson's Disease?
- PMID: 23882254
- PMCID: PMC3715734
- DOI: 10.3389/fneur.2013.00089
Is DOPA-Responsive Hypokinesia Responsible for Bimanual Coordination Deficits in Parkinson's Disease?
Abstract
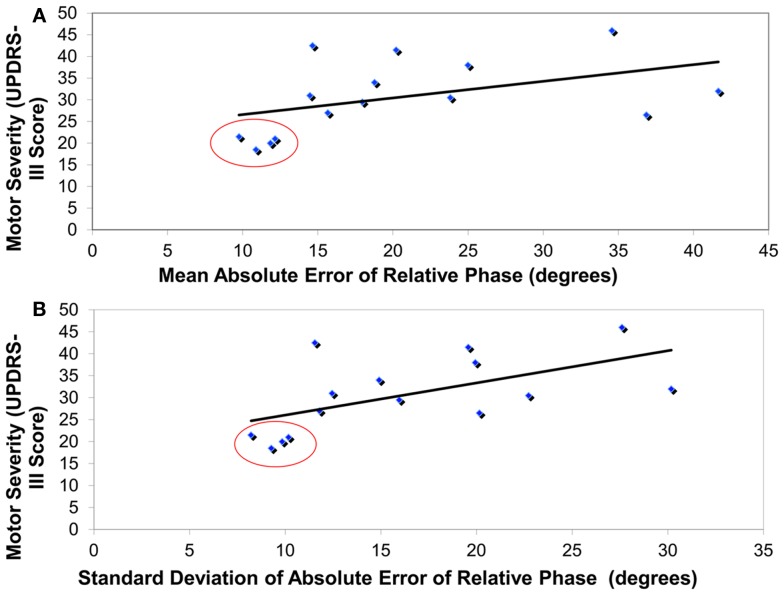
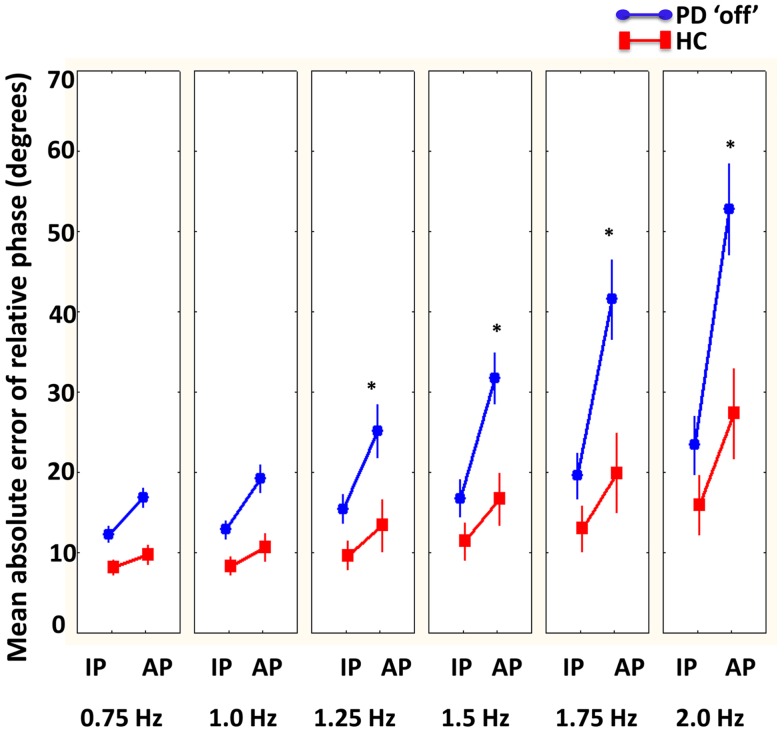
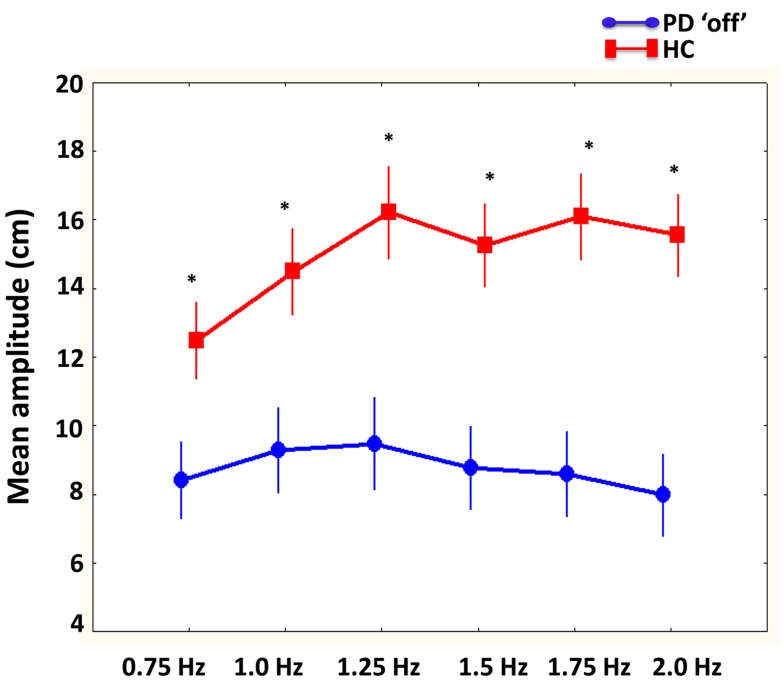
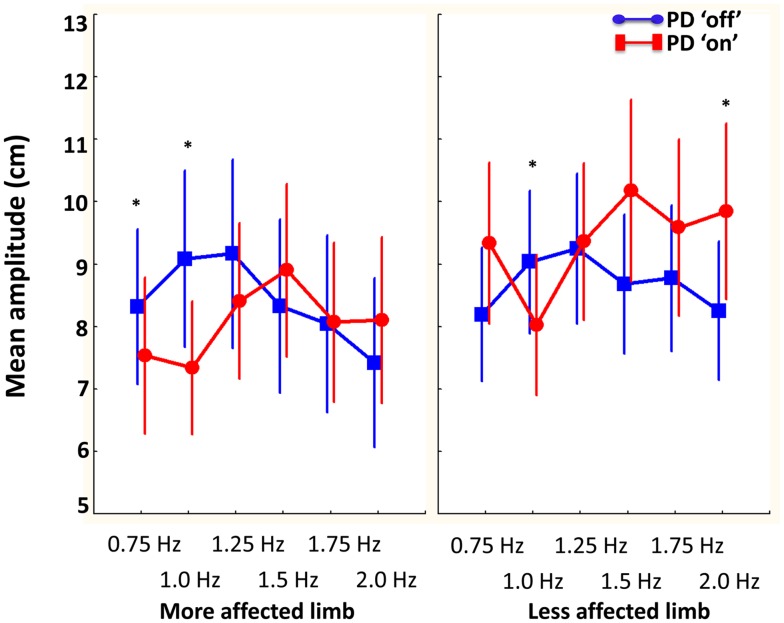
Bradykinesia is a well-documented DOPA-responsive clinical feature of Parkinson's disease (PD). While amplitude deficits (hypokinesia) are a key component of this slowness, it is important to consider how dopamine influences both the amplitude (hypokinesia) and frequency components of bradykinesia when a bimanually coordinated movement is required. Based on the notion that the basal ganglia are associated with sensory deficits, the influence of dopaminergic replacement on sensory feedback conditions during bimanual coordination was also evaluated. Bimanual movements were examined in PD and healthy comparisons in an unconstrained three-dimensional coordination task. PD were tested "off" (overnight withdrawal of dopaminergic treatment) and "on" (peak dose of dopaminergic treatment), while the healthy group was evaluated for practice effects across two sessions. Required cycle frequency (increased within each trial from 0.75 to 2 Hz), type of visual feedback (no vision, normal vision, and augmented vision), and coordination pattern (symmetrical in-phase and non-symmetrical anti-phase) were all manipulated. Overall, coordination (mean accuracy and standard deviation of relative phase) and amplitude deficits during bimanual coordination were confirmed in PD participants. In addition, significant correlations were identified between severity of motor symptoms as well as bradykinesia to greater coordination deficits (accuracy and stability) in PD "off" group. However, even though amplitude deficits (hypokinesia) improved with dopaminergic replacement, it did not improve bimanual coordination performance (accuracy or stability) in PD patients from "off" to "on." Interestingly, while coordination performance in both groups suffered in the augmented vision condition, the amplitude of the more affected limb of PD was notably influenced. It can be concluded that DOPA-responsive hypokinesia contributes to, but is not directly responsible for bimanual coordination impairments in PD. It is likely that bimanual coordination deficits in PD are caused by the combination of dopaminergic system dysfunction as well as other neural impairments that may be DOPA-resistant or related to non-dopaminergic pathways.
Keywords: Parkinson’s disease; bimanual coordination; bradykinesia; dopamine; hypokinesia; motor control disorders.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources