

Diabetic myonecrosis: a diagnostic challenge in patients with long-standing diabetes
- PMID: 23882392
- PMCID: PMC3716030
- DOI: 10.3402/jchimp.v3i1.20494
Diabetic myonecrosis: a diagnostic challenge in patients with long-standing diabetes
Abstract
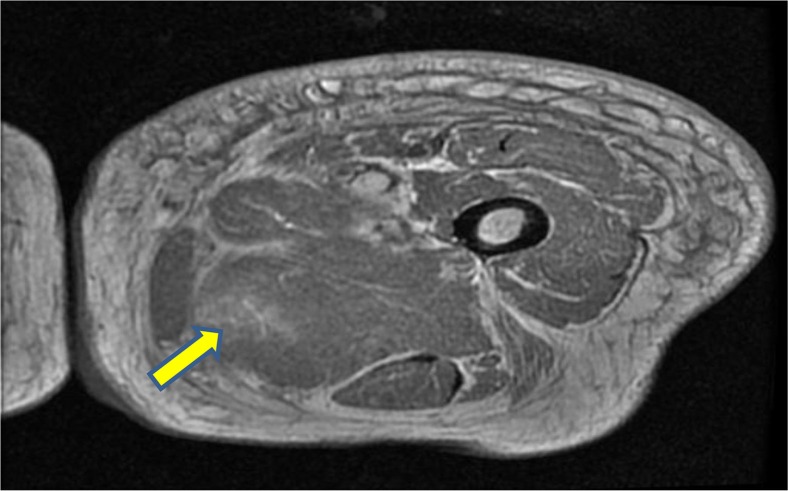
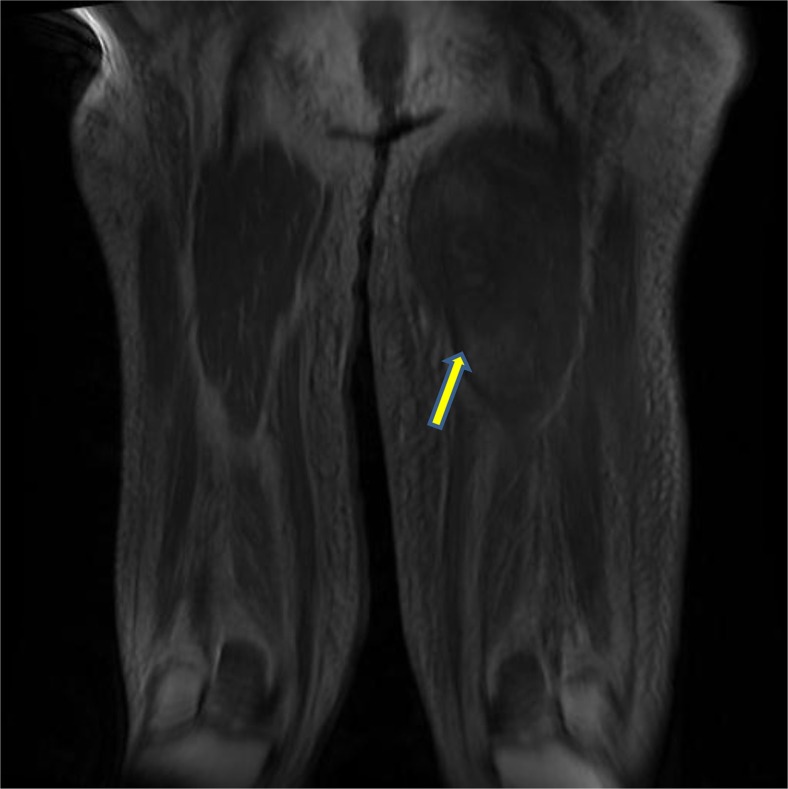
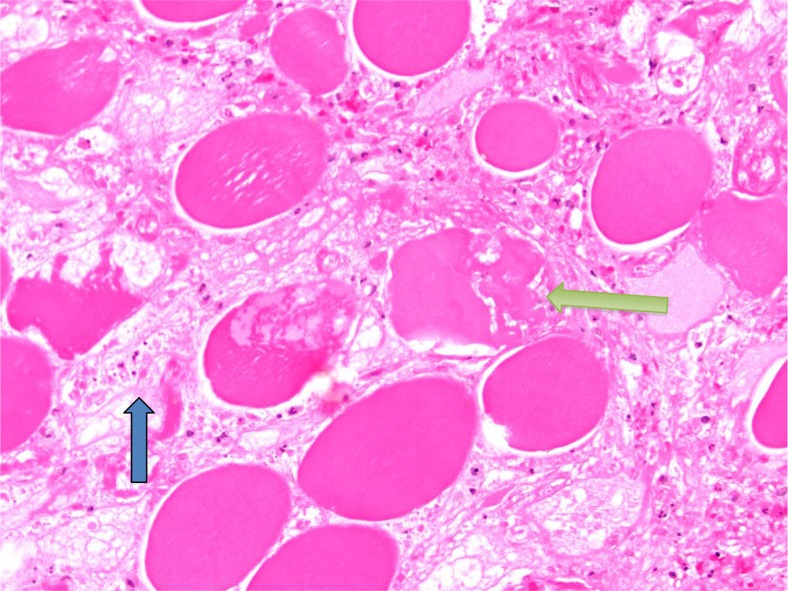
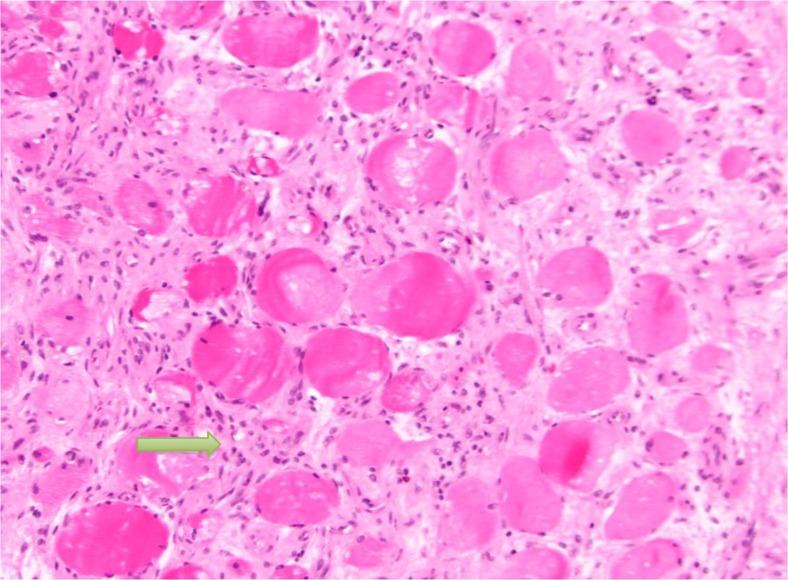
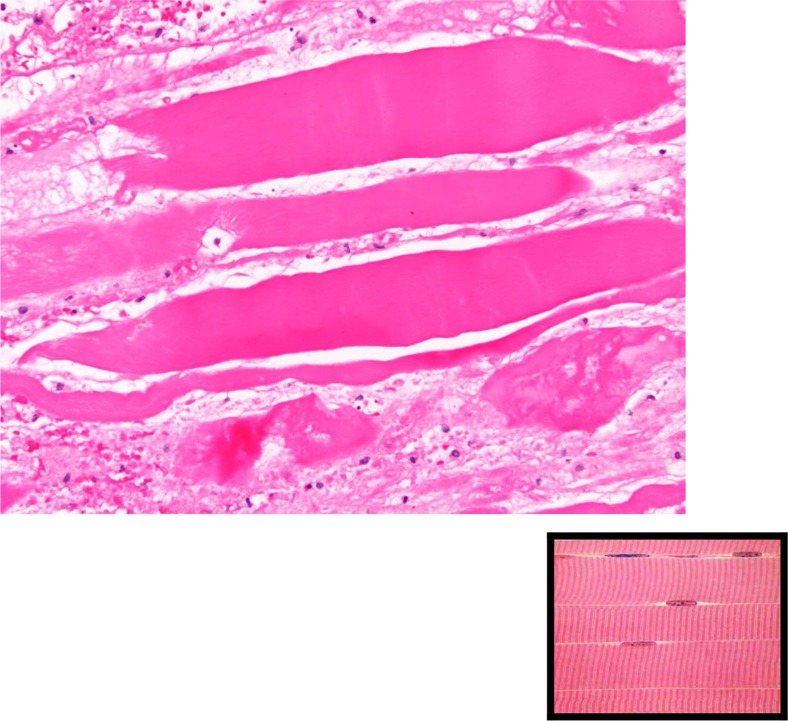
A 51-year-old female with a history of type 1 diabetes mellitus (DM) presented with sudden onset of pain and swelling of the left thigh. Her initial evaluation revealed mildly elevated erythrocyte sedimentation rate and creatine phosphokinase. Venous and arterial Doppler studies were negative for DVT and arterial thrombus. Further imaging with CT scan and then MRI revealed an irregular, enhancing space-occupying lesion of the left upper and mid-thigh. Subsequent muscle biopsy showed myonecrosis and proliferative myositis. Both findings are consistent with diabetic myonecrosis, which is a microvascular complication of long-standing poorly controlled DM. The patient was treated with analgesics, supportive care, and optimization of glycemic control. While short-term prognosis is good with adequate healing in a few weeks to several months, long-term prognosis is poor due to underlying extensive vascular disease. Although radiological findings are very suggestive of the diagnosis, most clinicians still need tissue biopsy to rule out other serious conditions such as infections and malignancy.
Keywords: diabetes mellitus; diabetic myonecrosis; microvascular complications; proliferative myositis.
Figures
References
-
- Angervall L, Stener B. Tumoriform focal muscular degeneration in two diabetic patients. Diabetologia. 1965;1:39–42.
-
- Galan A, Cowper SE, Bucala R. Nephrogenic systemic fibrosis (nephrogenic fibrosing dermopathy) Curr Opin Rheumatol. 2006;18(6):614–7. - PubMed
-
- Rashidi A, Bahrani O. Diabetic myonecrosis of the thigh. J Clin Endocrinol Metab. 2011;96(8):2310–1. - PubMed
-
- Hoyt JR, Wittich CM. Diabetic myonecrosis. J Clin Endocrinol Metab. 2008;93(10):3690. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources