

Association of MRI findings and visual outcome in idiopathic intracranial hypertension
- PMID: 23883223
- PMCID: PMC4048553
- DOI: 10.2214/AJR.12.9638
Association of MRI findings and visual outcome in idiopathic intracranial hypertension
Abstract
Objective: Patients with idiopathic intracranial hypertension (IIH) have elevated intracranial pressure (ICP) without an identifiable cause. The clinical course is variable, resulting in irreversible vision loss in some and a benign course in others. Although MRI findings have been described in IIH, their association with visual outcome has not been evaluated to date.
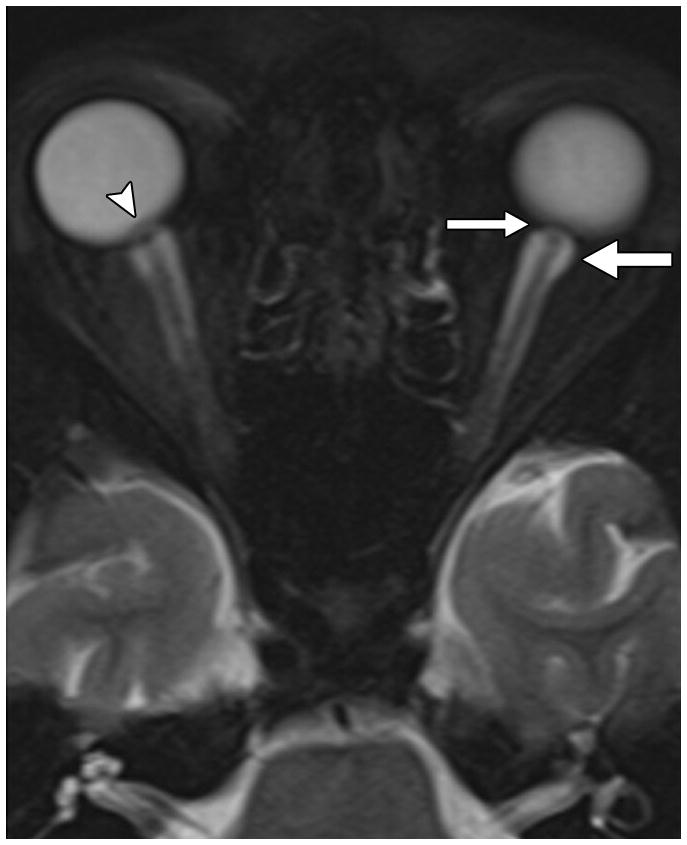
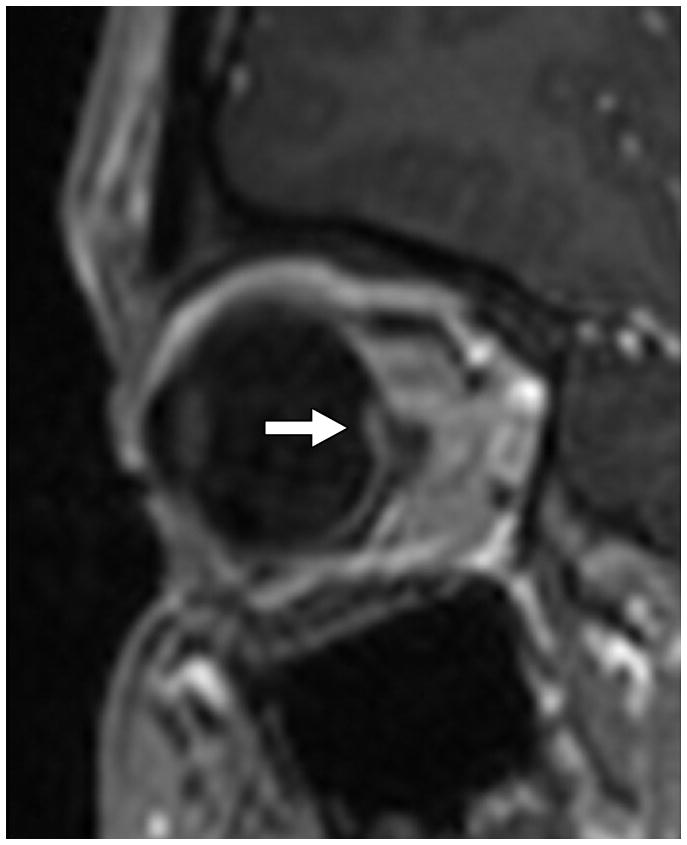
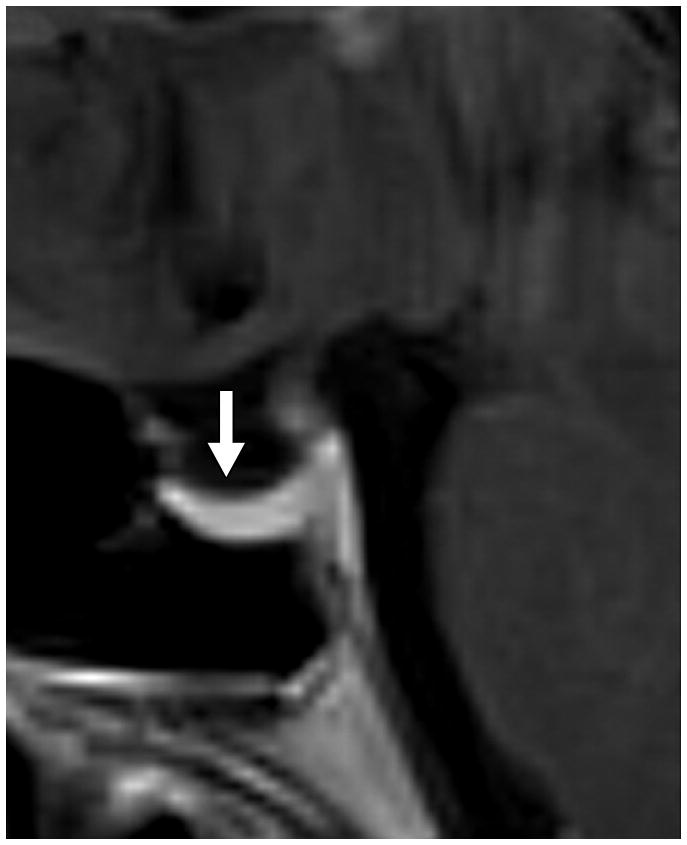
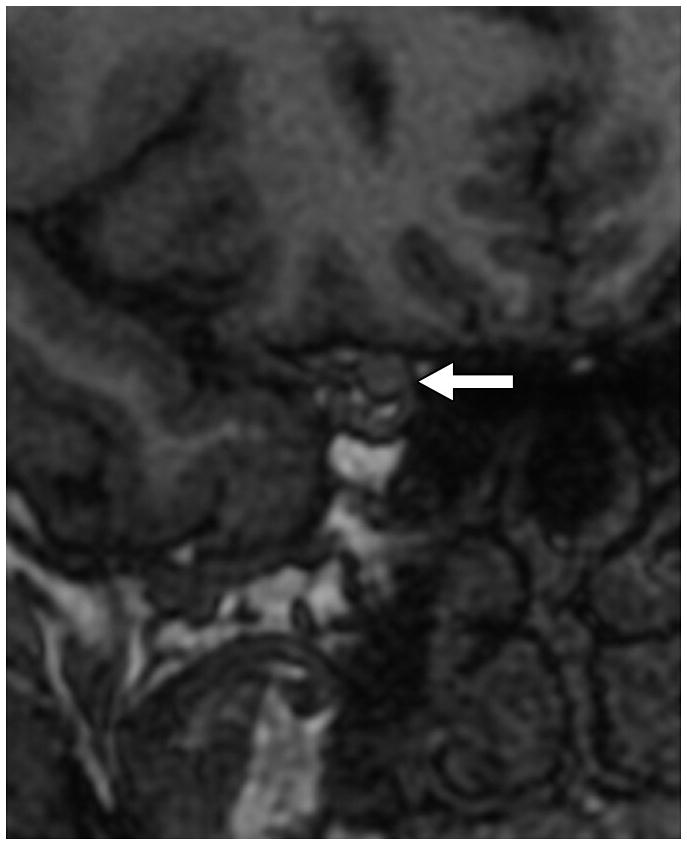
Materials and methods: Forty-six patients with IIH underwent funduscopic evaluation, visual field testing, lumbar puncture with opening pressure (OP) measurement, and MRI. Patients were stratified into the following groups by visual outcome: group 1, no vision loss (n = 28); group 2, some vision loss (n = 10); and group 3, severe vision loss (n = 8). MRI findings in the orbits, pituitary gland, and optic canals and the frequency of skull base cephaloceles and of transverse sinus (TS) stenosis were assessed by a reviewer blinded to the patients' visual outcome. Demographic, clinical, and MRI findings were evaluated for association with visual outcome.
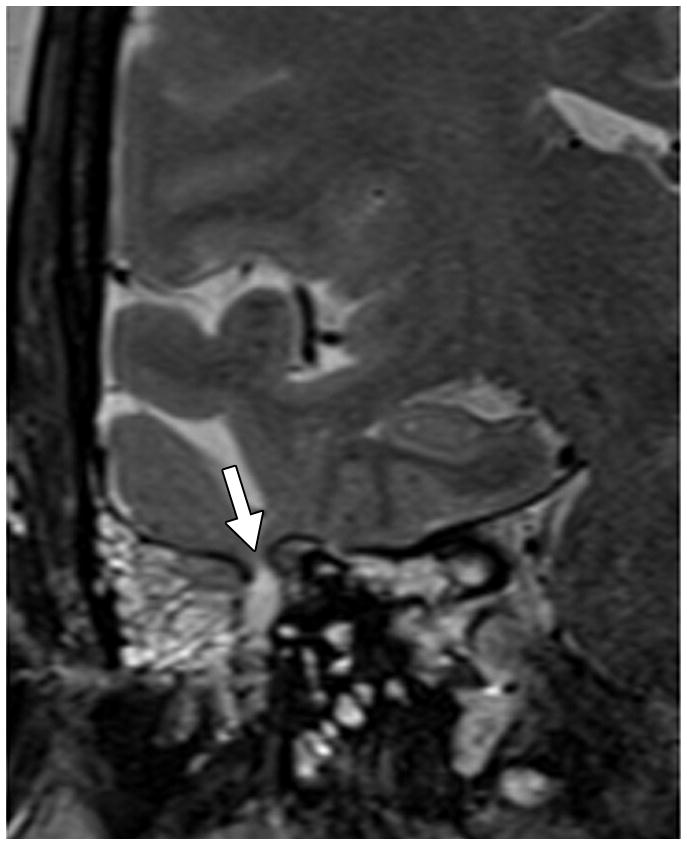
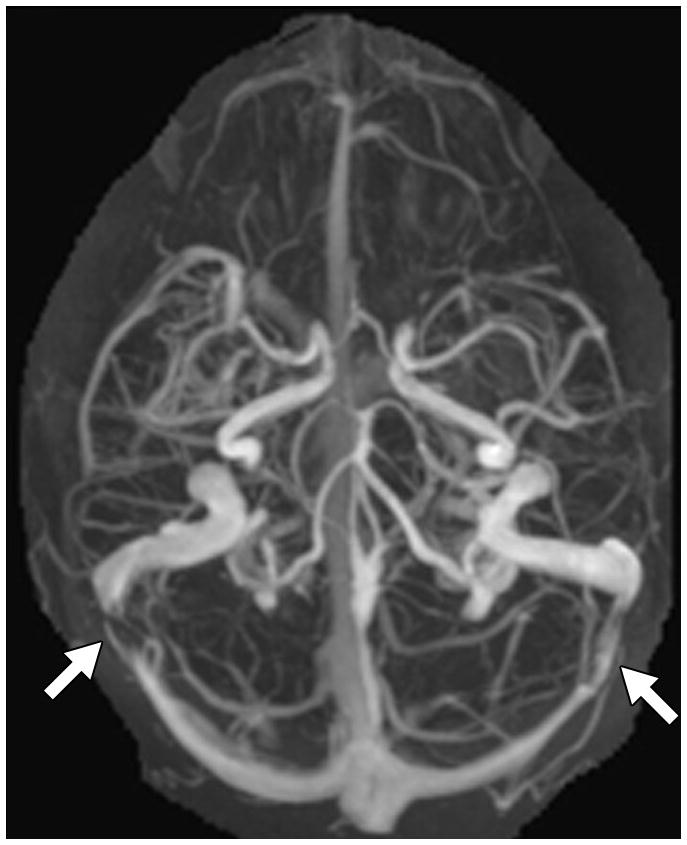
Results: Patients in group 3 (worst visual outcome) were significantly younger (p = 0.03) and had higher OP (p = 0.04) than patients in the other groups. There were no significant differences in sex, race, or body mass index. Despite worse visual outcomes and sometimes fulminant vision loss, there were no differences in the frequency of orbital MRI findings or TS stenosis, optic canal diameter, and pituitary appearance among the three groups. Group 3 had significantly lower cephalocele frequency than the other groups (p = 0.04).
Conclusion: Although MRI findings may suggest elevated ICP and the diagnosis of IIH, they are not predictive of visual outcome in patients with IIH.
Conflict of interest statement
Figures
Similar articles
-
Thinning of the Skull Base and Calvarial Thickness in Patients With Idiopathic Intracranial Hypertension.J Neuroophthalmol. 2022 Jun 1;42(2):192-198. doi: 10.1097/WNO.0000000000001504. Epub 2022 Feb 15. J Neuroophthalmol. 2022. PMID: 35195543
-
Idiopathic Intracranial Hypertension in a pubertal paediatric Indian patient.Nepal J Ophthalmol. 2017 Jan;9(18):74-78. doi: 10.3126/nepjoph.v9i1.17539. Nepal J Ophthalmol. 2017. PMID: 29022960
-
Non-invasive assessment of intracranial compliance in idiopathic intracranial hypertension: an MRI-ICP study.Eye (Lond). 2025 May;39(7):1309-1317. doi: 10.1038/s41433-024-03547-7. Epub 2025 Jan 24. Eye (Lond). 2025. PMID: 39856425 Free PMC article.
-
Fulminant Idiopathic Intracranial Hypertension.Curr Neurol Neurosci Rep. 2020 Mar 26;20(4):8. doi: 10.1007/s11910-020-1026-8. Curr Neurol Neurosci Rep. 2020. PMID: 32219578 Review.
-
A systematic review of surgical treatments of idiopathic intracranial hypertension (IIH).Neurosurg Rev. 2021 Apr;44(2):773-792. doi: 10.1007/s10143-020-01288-1. Epub 2020 Apr 25. Neurosurg Rev. 2021. PMID: 32335853
Cited by
-
Inaccuracy of idiopathic intracranial hypertension diagnosis in case reports.Eye (Lond). 2023 Oct;37(15):3243-3248. doi: 10.1038/s41433-023-02499-8. Epub 2023 Mar 16. Eye (Lond). 2023. PMID: 36928224 Free PMC article. Review.
-
Clinical and Neuro-ophthalmologic Predictors of Visual Outcome in Idiopathic Intracranial Hypertension.Neuroophthalmology. 2018 Jan 9;42(4):201-208. doi: 10.1080/01658107.2017.1400570. eCollection 2018 Aug. Neuroophthalmology. 2018. PMID: 30042789 Free PMC article.
-
Meningoceles in idiopathic intracranial hypertension.AJR Am J Roentgenol. 2014 Mar;202(3):608-13. doi: 10.2214/AJR.13.10874. AJR Am J Roentgenol. 2014. PMID: 24555598 Free PMC article.
-
Quantitative parameters for diagnosis of idiopathic intracranial hypertension on brain MRI.Eur J Radiol Open. 2021 Aug 26;8:100371. doi: 10.1016/j.ejro.2021.100371. eCollection 2021. Eur J Radiol Open. 2021. PMID: 34485627 Free PMC article.
-
Idiopathic intracranial hypertension: Imaging and clinical fundamentals.World J Radiol. 2024 Dec 28;16(12):722-748. doi: 10.4329/wjr.v16.i12.722. World J Radiol. 2024. PMID: 39801664 Free PMC article. Review.
References
-
- Friedman DI, Jacobson DM. Diagnostic criteria for idiopathic intracranial hypertension. Neurology. 2002;59:1492–1495. - PubMed
-
- Giuseffi V, Wall M, Siegel PZ, Rojas PB. Symptoms and disease associations in idiopathic intracranial hypertension (pseudotumor cerebri): a case-control study. Neurology. 1991;41:239–244. - PubMed
-
- Corbett JJ, Savino PJ, Thompson HS, et al. Visual loss in pseudotumor cerebri. Follow-up of 57 patients from five to 41 years and a profile of 14 patients with permanent severe visual loss. Arch Neurol. 1982;39:461–474. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
