

Vaginal breech delivery: results of a prospective registration study
- PMID: 23883361
- PMCID: PMC3728003
- DOI: 10.1186/1471-2393-13-153
Vaginal breech delivery: results of a prospective registration study
Abstract
Background: Most countries recommend planned cesarean section in breech deliveries, which is considered safer than vaginal delivery. As one of few countries in the western world Norway has continued to practice planned vaginal delivery in selected women. The aim of this study is to evaluate prospectively registered neonatal and maternal outcomes in term singleton breech deliveries in a Norwegian hospital during a ten years period. We aim to compare maternal and neonatal outcomes in term breech pregnancies subjected either to planned vaginal or elective cesarean section.
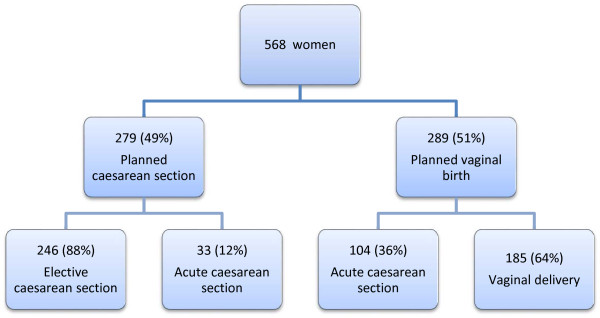
Methods: A prospective registration study including 568 women with term breech deliveries (>37 weeks) consecutively registered at Sorlandet Hospital Kristiansand between 2001 and 2011. Fetal and maternal outcomes were compared according to delivery method; planned vaginal delivery versus planned cesarean section.
Results: Of 568 women, elective cesarean section was planned in 279 (49%) cases and vaginal delivery was planned in 289 (51%) cases. Acute cesarean section was performed in 104 of the planned vaginal deliveries (36.3%). There were no neonatal deaths. Two cases of serious neonatal morbidity were reported in the planned vaginal group. One infant had seizures, brachial plexus injury, and cephalhematoma. The other infant had 5-minutes Apgar < 4. Twenty-nine in the planned vaginal group (10.0%) and eight in the planned cesarean section group (2.9%) (p < 0.001) were transferred to the neonatal intensive care unit. However, only one infant was admitted for ≥4 days. According to follow-up data (median six years) none of these infants had long-term sequelae. Regarding maternal morbidity, blood loss was the only variable that was significantly higher in the planned cesarean section group versus in the vaginal delivery group (p < 0.001).
Conclusions: Strict guidelines were followed in all cases. There were no neonatal deaths. Two infants had serious neonatal morbidity in the planned vaginal group without long-term sequelae.
Similar articles
-
Planned vaginal delivery versus elective caesarean section in singleton term breech presentation: a study of 1116 cases.Eur J Obstet Gynecol Reprod Biol. 2001 Oct;98(2):186-92. doi: 10.1016/s0301-2115(01)00333-5. Eur J Obstet Gynecol Reprod Biol. 2001. PMID: 11574129
-
[Breech Presentation: CNGOF Guidelines for Clinical Practice - Benefits and Risks for the Neonate and Child of Planned Vaginal Delivery versus Elective Cesarean Section].Gynecol Obstet Fertil Senol. 2020 Jan;48(1):95-108. doi: 10.1016/j.gofs.2019.10.023. Epub 2019 Oct 31. Gynecol Obstet Fertil Senol. 2020. PMID: 31678508 Review. French.
-
Neonatal outcome of singleton term breech deliveries in Norway from 1991 to 2011.Acta Obstet Gynecol Scand. 2015 Sep;94(9):997-1004. doi: 10.1111/aogs.12684. Epub 2015 Jun 24. Acta Obstet Gynecol Scand. 2015. PMID: 26037909
-
Maternal and neonatal short-term outcome after vaginal breech delivery >36 weeks of gestation with and without MRI-based pelvimetric measurements: a Hannover retrospective cohort study.J Perinat Med. 2024 Dec 24;53(3):316-326. doi: 10.1515/jpm-2024-0173. Print 2025 Mar 26. J Perinat Med. 2024. PMID: 39711256
-
The risks of planned vaginal breech delivery versus planned caesarean section for term breech birth: a meta-analysis including observational studies.BJOG. 2016 Jan;123(1):49-57. doi: 10.1111/1471-0528.13524. Epub 2015 Jul 29. BJOG. 2016. PMID: 26234485 Review.
Cited by
-
Cardiotocography in breech versus vertex delivery: an examiner-blinded, cross-sectional nested case-control study.BMC Pregnancy Childbirth. 2016 Oct 21;16(1):319. doi: 10.1186/s12884-016-1115-5. BMC Pregnancy Childbirth. 2016. PMID: 27769196 Free PMC article.
-
[Breech vaginal delivery: a study of maternal and neonatal morbidity and mortality].Pan Afr Med J. 2014 Jan 17;17:27. doi: 10.11604/pamj.2014.17.27.2037. eCollection 2014. Pan Afr Med J. 2014. PMID: 24932338 Free PMC article. French.
-
Intra- and inter-rater reliability in a comparative study of cross-sectional and spiral computed tomography pelvimetry methods.Acta Radiol Open. 2019 Jun 11;8(6):2058460119855187. doi: 10.1177/2058460119855187. eCollection 2019 Jun. Acta Radiol Open. 2019. PMID: 31218082 Free PMC article.
-
Maternal and neonatal outcome after vaginal breech delivery at term of children weighing more or less than 3.8 kg: A FRABAT prospective cohort study.PLoS One. 2018 Aug 23;13(8):e0202760. doi: 10.1371/journal.pone.0202760. eCollection 2018. PLoS One. 2018. PMID: 30138358 Free PMC article.
-
Maternal and fetal risks of planned vaginal breech delivery vs planned caesarean section for term breech birth: A systematic review and meta-analysis.J Glob Health. 2022 Jul 16;12:04055. doi: 10.7189/jogh.12.04055. J Glob Health. 2022. PMID: 35976004 Free PMC article.
References
-
- Hannah ME, Hannah WJ, Hewson SA, Hodnett ED, Saigal S, Willan AR. Planned caesarean section versus planned vaginal birth for breech presentation at term: a randomised multicentre trial. Term Breech Trial Collaborative Group. Lancet. 2000;356:1375–1383. doi: 10.1016/S0140-6736(00)02840-3. - DOI - PubMed
-
- Van RJ, Rosendaal F. There is still room for disagreement about vaginal delivery of breech infants at term. BJOG. 2002;109:967–969. - PubMed
-
- Daviss BA, Johnson KC, Lalonde AB. Evolving evidence since the term breech trial: Canadian response, European dissent, and potential solutions. J Obstet Gynaecol Can. 2010;32:217–224. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
