

Low-flow CO₂ removal integrated into a renal-replacement circuit can reduce acidosis and decrease vasopressor requirements
- PMID: 23883472
- PMCID: PMC4056563
- DOI: 10.1186/cc12833
Low-flow CO₂ removal integrated into a renal-replacement circuit can reduce acidosis and decrease vasopressor requirements
Abstract
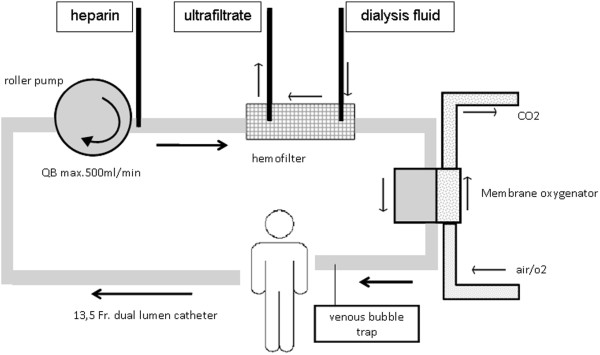
Introduction: Lung-protective ventilation in patients with ARDS and multiorgan failure, including renal failure, is often paralleled with a combined respiratory and metabolic acidosis. We assessed the effectiveness of a hollow-fiber gas exchanger integrated into a conventional renal-replacement circuit on CO₂ removal, acidosis, and hemodynamics.
Methods: In ten ventilated critically ill patients with ARDS and AKI undergoing renal- and respiratory-replacement therapy, effects of low-flow CO₂ removal on respiratory acidosis compensation were tested by using a hollow-fiber gas exchanger added to the renal-replacement circuit. This was an observational study on safety, CO₂-removal capacity, effects on pH, ventilator settings, and hemodynamics.
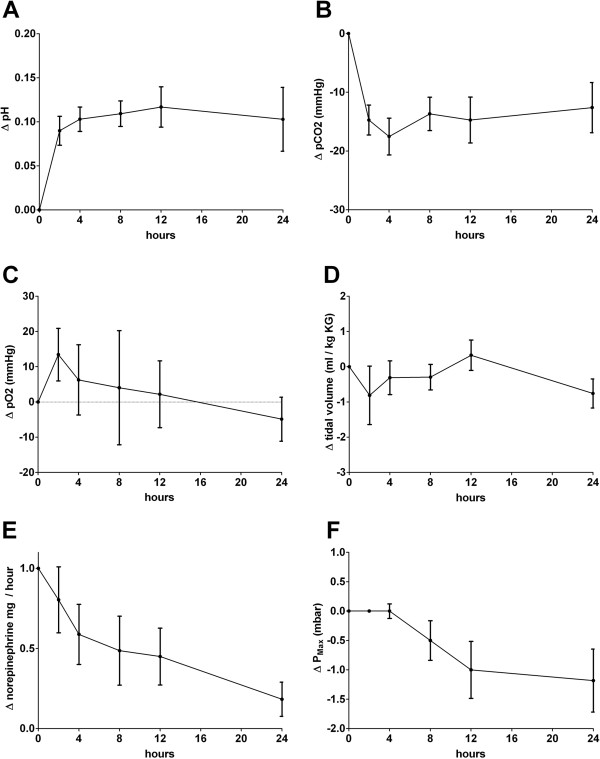
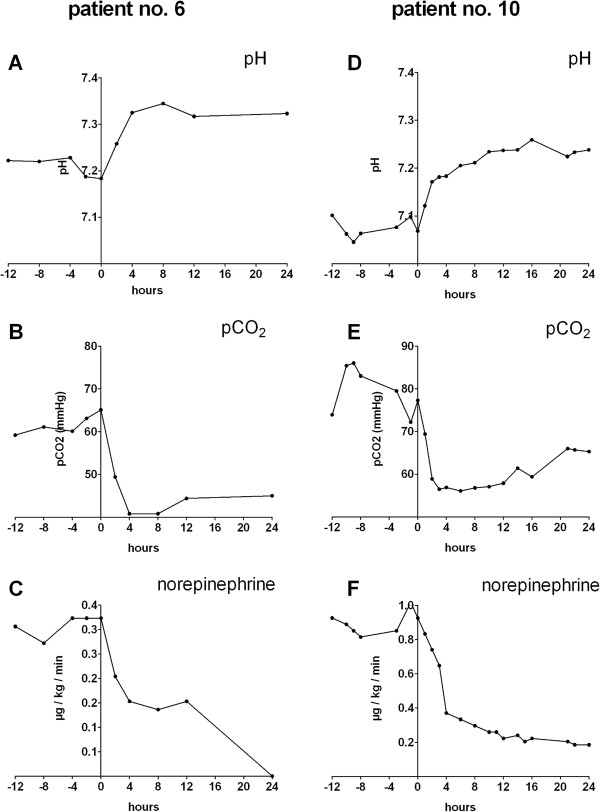
Results: CO₂ elimination in the low-flow circuit was safe and was well tolerated by all patients. After 4 hours of treatment, a mean reduction of 17.3 mm Hg (-28.1%) pCO₂ was observed, in line with an increase in pH. In hemodynamically instable patients, low-flow CO₂ elimination was paralleled by hemodynamic improvement, with an average reduction of vasopressors of 65% in five of six catecholamine-dependent patients during the first 24 hours.
Conclusions: Because no further catheters are needed, besides those for renal replacement, the implementation of a hollow-fiber gas exchanger in a renal circuit could be an attractive therapeutic tool with only a little additional trauma for patients with mild to moderate ARDS undergoing invasive ventilation with concomitant respiratory acidosis, as long as no severe oxygenation defects indicate ECMO therapy.
Figures
References
-
- Amato MB, Barbas CS, Medeiros DM, Magaldi RB, Schettino GP, Lorenzi-Filho G, Kairalla RA, Deheinzelin D, Munoz C, Oliveira R, Takagaki TY, Carvalho CR. Effect of a protective-ventilation strategy on mortality in the acute respiratory distress syndrome. N Engl J Med. 1998;17(6):347–354. doi: 10.1056/NEJM199802053380602. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
