

Extracranial glioblastoma with synchronous metastases in the lung, pulmonary lymph nodes, vertebrae, cervical muscles and epidural space in a young patient - case report and review of literature
- PMID: 23883669
- PMCID: PMC3726502
- DOI: 10.1186/1756-0500-6-290
Extracranial glioblastoma with synchronous metastases in the lung, pulmonary lymph nodes, vertebrae, cervical muscles and epidural space in a young patient - case report and review of literature
Abstract
Background: Extraneural and extracranial metastases of glioblastoma (GB) are very rarely reported in the literature. They occur in only 0.2% of all GB patients.
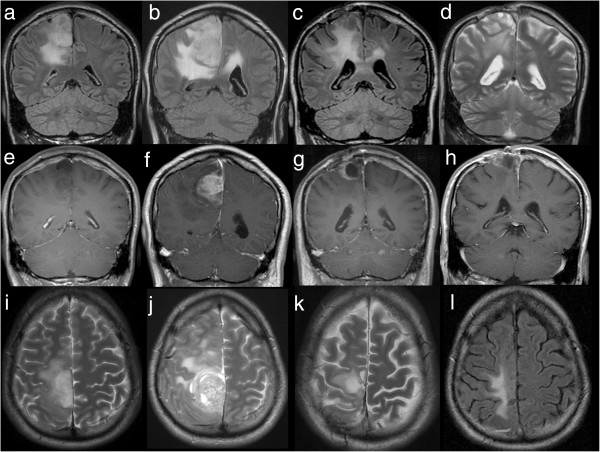
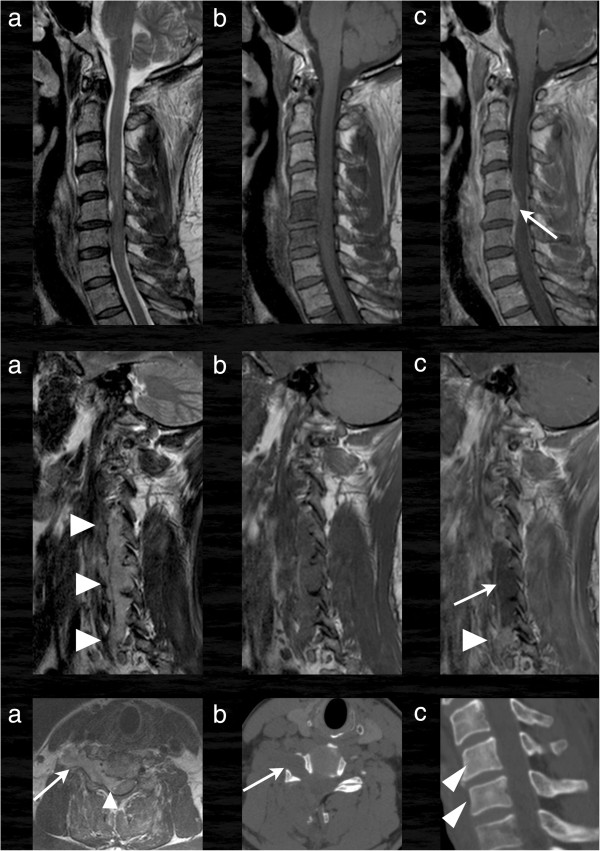
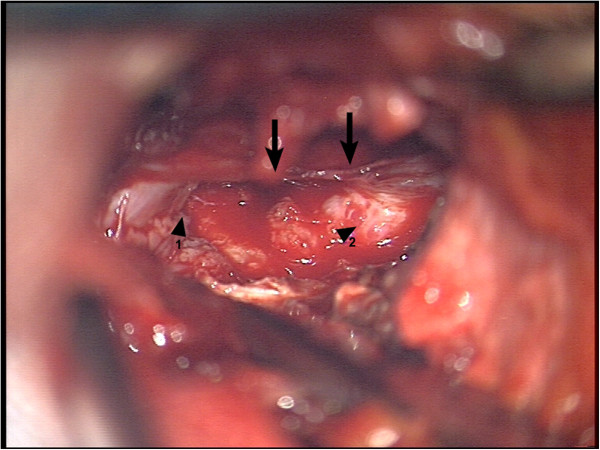
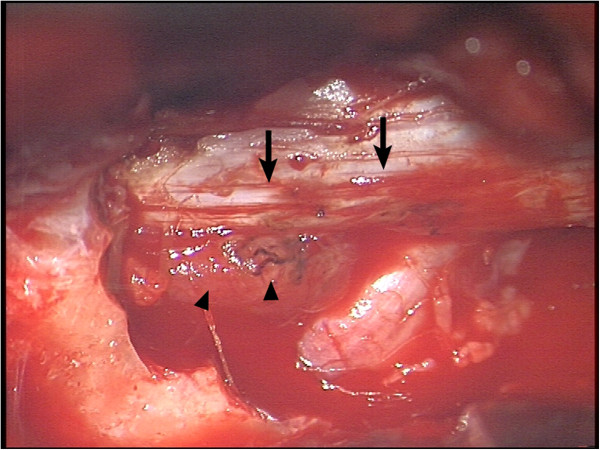
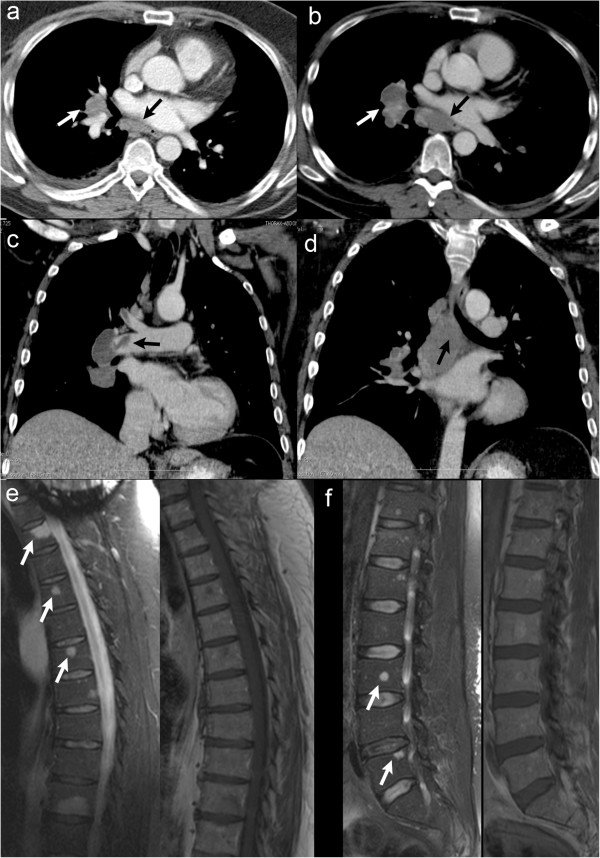
Case presentation: We present a 40 year old caucasian male with secondary GB and first diagnosis of an astrocytoma world health organisation (WHO) grade II through stereotactic biopsy in 2006. He presented a new hemiparesis and a progress of the known mass lesion in 2008. Subtotal tumor resection was performed and the histological examination verified a GB. After combined radio- and chemotherapy the adjuvant temozolomide therapy was not started because of non-compliance. In 2011 a second local relapse was resected and 4 month later the patient presented a fast progressing tetraparesis. Cervical CT and MRI scan showed a mass lesion infiltrating the fifth and sixth vertebra with infiltration of the spinal canal and large paravertebral tumor masses. Emergency surgery was performed. By additional screening further metastases were detected in the thoracal and lumbal spine and surprisingly also in the lung and pulmonary lymphnodes. Palliative radio- and chemotherapy of the pulmonal lesions was completed, further antitumor therapy was rejected. The patient died 10 months after diagnosis of the extraneural metastases.
Conclusion: Especially young "long-term-survivors" seem to have a higher risk of extraneural metastasis from a GB and appropriate staging should be performed in these cases.
Figures
Similar articles
-
Diagnosis and Management of Spinal Metastasis of Glioblastoma.Can J Neurol Sci. 2015 Nov;42(6):410-3. doi: 10.1017/cjn.2015.285. Epub 2015 Aug 27. Can J Neurol Sci. 2015. PMID: 26310615
-
Meningeal seeding from glioblastoma multiforme treated with radiotherapy and temozolomide.Asian J Surg. 2017 Jan;40(1):61-65. doi: 10.1016/j.asjsur.2013.07.012. Epub 2013 Aug 23. Asian J Surg. 2017. PMID: 23978432
-
Extra central nervous system metastases from cerebral glioblastoma multiforme in elderly patients. Clinico-pathological remarks on our series of seven cases and critical review of the literature.Tumori. 2008 Jan-Feb;94(1):40-51. doi: 10.1177/030089160809400109. Tumori. 2008. PMID: 18468334
-
Solitary vertebral metastatic glioblastoma in the absence of primary brain tumor relapse: a case report and literature review.BMC Med Imaging. 2020 Jul 31;20(1):89. doi: 10.1186/s12880-020-00488-x. BMC Med Imaging. 2020. PMID: 32736607 Free PMC article. Review.
-
Subcutaneous tissue metastasis from glioblastoma multiforme: A case report and review of the literature.Neurocirugia (Engl Ed). 2019 May-Jun;30(3):149-154. doi: 10.1016/j.neucir.2018.03.005. Epub 2018 May 16. Neurocirugia (Engl Ed). 2019. PMID: 29778285 Review. English, Spanish.
Cited by
-
Case report of pulmonary metastasis in a male Wistar rat glioblastoma model.J Toxicol Pathol. 2021 Jan;34(1):95-99. doi: 10.1293/tox.20-0034. Epub 2020 Dec 19. J Toxicol Pathol. 2021. PMID: 33627949 Free PMC article.
-
Increasing C-reactive protein levels in a patient with glioblastoma with lymph node metastasis: a case report.BMC Neurol. 2023 Oct 4;23(1):354. doi: 10.1186/s12883-023-03402-4. BMC Neurol. 2023. PMID: 37794336 Free PMC article.
-
A case series of extraneural metastatic glioblastoma at Memorial Sloan Kettering Cancer Center.Neurooncol Pract. 2021 Feb 3;8(3):325-336. doi: 10.1093/nop/npaa083. eCollection 2021 Jun. Neurooncol Pract. 2021. PMID: 34055380 Free PMC article.
-
Extracranial metastasis of glioblastoma with genomic analysis: a case report and review of the literature.Transl Cancer Res. 2022 Aug;11(8):2917-2925. doi: 10.21037/tcr-22-955. Transl Cancer Res. 2022. PMID: 36093544 Free PMC article.
-
Extracranial Metastases of a Cerebral Glioblastoma: A Case Report and Review of the Literature.Case Rep Oncol. 2018 Aug 28;11(2):591-600. doi: 10.1159/000492111. eCollection 2018 May-Aug. Case Rep Oncol. 2018. PMID: 30283316 Free PMC article.
References
-
- Piccirilli M, Brunetto GM, Rocchi G, Giangaspero F, Salvati M. Extra central nervous system metastases from cerebral glioblastoma multiforme in elderly patients. Clinico-pathological remarks on our series of seven cases and critical review of the literature. Tumori. 2008;94(1):40–51. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
