

Asthma and atopic dermatitis are associated with increased risk of clinical Plasmodium falciparum malaria
- PMID: 23883878
- PMCID: PMC3731724
- DOI: 10.1136/bmjopen-2013-002835
Asthma and atopic dermatitis are associated with increased risk of clinical Plasmodium falciparum malaria
Abstract
Objectives: To assess the impact of atopy and allergy on the risk of clinical malaria.
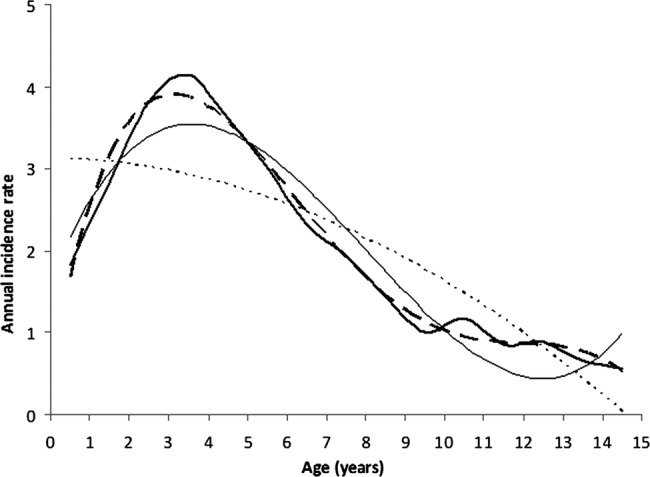
Design: A clinical and immunological allergy cross-sectional survey in a birth cohort of 175 children from 1 month to 14 years of age followed for up to 15 years in a longitudinal open cohort study of malaria in Senegal. Malaria incidence data were available for 143 of these children (aged 4 months to 14 years of age) for up to 15 years. Mixed-model regression analysis was used to determine the impact of allergy status on malaria incidence, adjusting for age, gender, sickle-cell trait and force of infection.
Main outcome measures: Asthma, allergic rhinoconjunctivitis and atopic dermatitis status, the number of clinical Plasmodium falciparum malaria episodes since birth and associated parasite density.
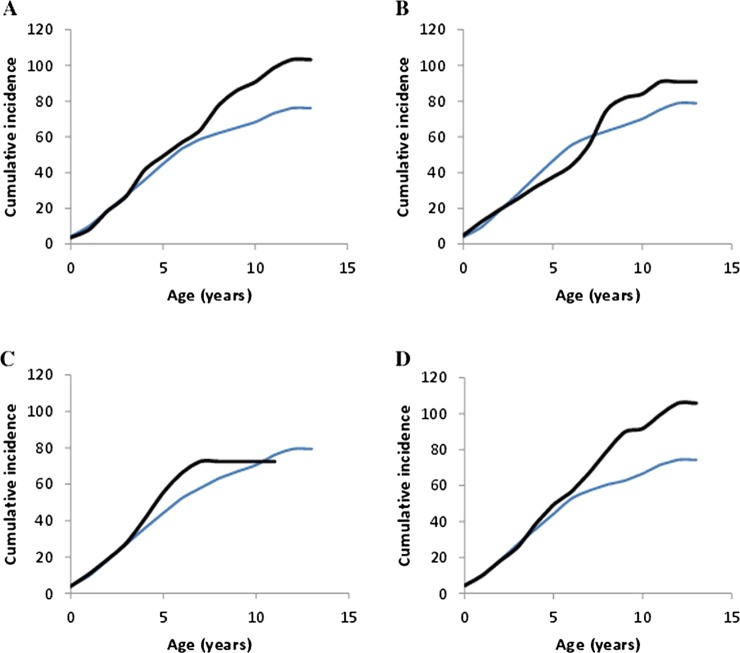
Results: 12% of the children were classified as asthmatic and 10% as having atopic dermatitis. These groups had respectively a twofold (OR 2.12 95%; CI 1.46 to 3.08; p=8×10(-5)) and threefold (OR 3.15; 1.56 to 6.33; p=1.3×10(-3)) increase in the risk of clinical P falciparum malaria once older than the age of peak incidence of clinical malaria (3-4 years of age). They also presented with higher P falciparum parasite densities (asthma: mean 105.3 parasites/μL±SE 41.0 vs 51.3±9.7; p=6.2×10(-3). Atopic dermatitis: 135.4±70.7 vs 52.3±11.0; p=0.014). There was no effect of allergy on the number of non-malaria clinical presentations. Individuals with allergic rhinoconjunctivitis did not have an increased risk of clinical malaria nor any difference in parasite densities.
Conclusions: These results demonstrate that asthma and atopic dermatitis delay the development of clinical immunity to P falciparum. Despite the encouraging decrease in malaria incidence rates in Africa, a significant concern is the extent to which the increase in allergy will exacerbate the burden of malaria. Given the demonstrated antiparasitic effect of antihistamines, administration to atopic children will likely reduce the burden of clinical malaria in these children, increase the efficacy of first-line treatment antimalarials and alleviate the non-infectious consequences of atopy.
Figures
References
-
- WAO World Allergy Organization, 2010. http://www.worldallergy.org/index.php
-
- Asher MI, Montefort S, Björkstén B, et al. Worldwide time trends in the prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and eczema in childhood: ISAAC phases one and three repeat multicountry cross-sectional surveys. Lancet 2006;368:733–43 - PubMed
-
- Mosmann TR, Coffman RL. TH1 and TH2 cells: different patterns of lymphokine secretion lead to different functional properties. Ann Rev Immunol 1989;7:145–73 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources