

Responsiveness to reduced dosage of rituximab in Chinese patients with neuromyelitis optica
- PMID: 23884041
- PMCID: PMC3776460
- DOI: 10.1212/WNL.0b013e3182a1aac7
Responsiveness to reduced dosage of rituximab in Chinese patients with neuromyelitis optica
Abstract
Objective: To determine the effect of a lower dose of rituximab in depleting B lymphocytes, maintaining low B-cell counts, and relapse in patients with neuromyelitis optica (NMO) and NMO spectrum disorders.
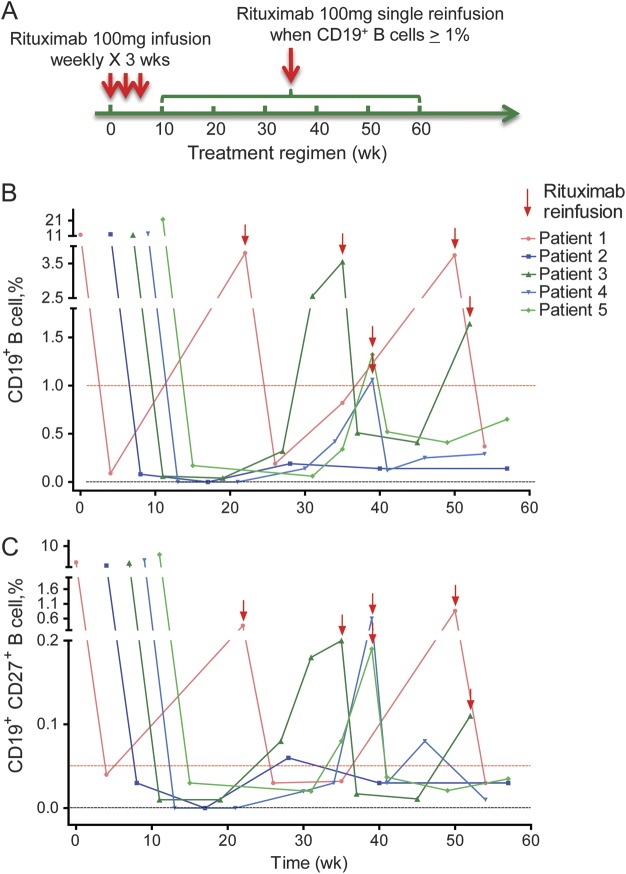
Methods: We treated 5 Chinese patients with deteriorating NMO and NMO spectrum disorders with a 100-mg IV infusion of rituximab once a week for 3 consecutive weeks, followed by additional infusion of the same dosage depending on circulating B-cell repopulation.
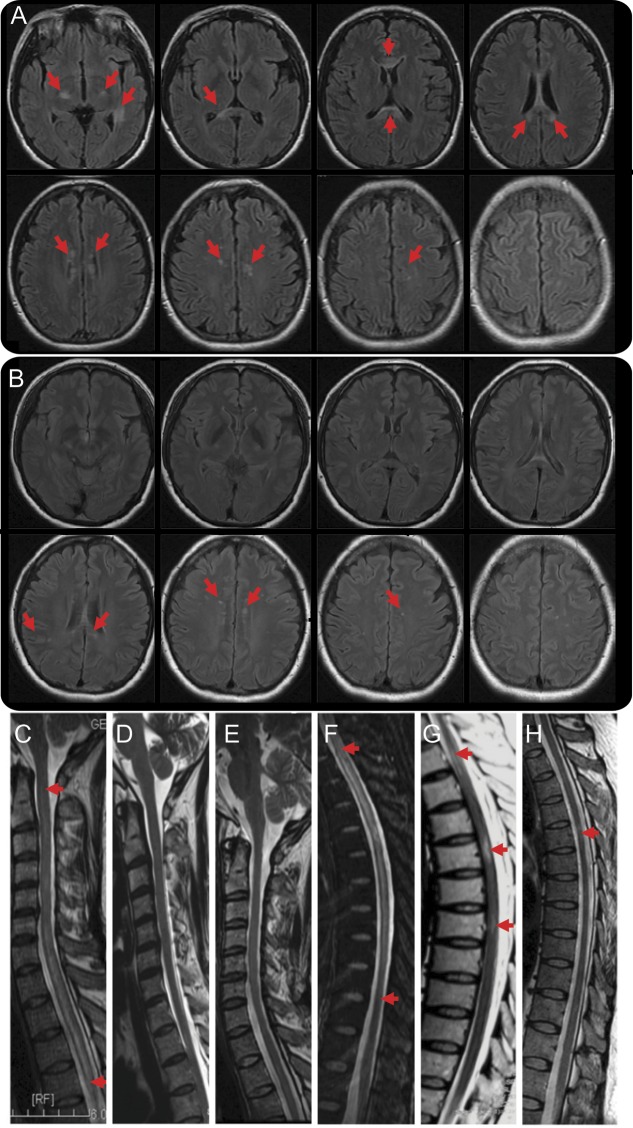
Results: This reduced dosage of rituximab was sufficient to deplete B cells and maintain low B-cell counts. None of the treated patients experienced relapse, and all patients exhibited stabilized or improved neurologic function during the 1-year follow-up period. MRI revealed the absence of new lesions, no enhancement in spinal cord and brain, a significant shrinkage of spinal cord segments, and a reduction/disappearance of previous brain lesions.
Conclusion: A lower dosage of rituximab may be sufficient in depleting B cells, maintaining low B-cell counts, and preventing disease progression in Chinese patients with NMO.
Figures
Comment in
-
Responsiveness to reduced dosage of rituximab in Chinese patients with neuromyelitis optica.Neurology. 2014 Feb 11;82(6):546-7. doi: 10.1212/01.wnl.0000444161.12981.ba. Neurology. 2014. PMID: 24514012 No abstract available.
-
Responsiveness to reduced dosage of rituximab in Chinese patients with neuromyelitis optica.Neurology. 2014 Feb 11;82(6):547. Neurology. 2014. PMID: 24672810 No abstract available.
-
Author response.Neurology. 2014 Feb 11;82(6):547. Neurology. 2014. PMID: 24672811 No abstract available.
References
-
- Bedi GS, Brown AD, Delgado SR, Usmani N, Lam BL, Sheremata WA. Impact of rituximab on relapse rate and disability in neuromyelitis optica. Mult Scler 2011;17:1225–1230 - PubMed
-
- Cree BA, Lamb S, Morgan K, Chen A, Waubant E, Genain C. An open label study of the effects of rituximab in neuromyelitis optica. Neurology 2005;64:1270–1272 - PubMed
-
- Greenberg BM, Graves D, Remington G, et al. Rituximab dosing and monitoring strategies in neuromyelitis optica patients: creating strategies for therapeutic success. Mult Scler 2012;18:1022–1026 - PubMed
-
- Jacob A, Weinshenker BG, Violich I, et al. Treatment of neuromyelitis optica with rituximab: retrospective analysis of 25 patients. Arch Neurol 2008;65:1443–1448 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources