

Low rates of adherence for tumor necrosis factor-α inhibitors in Crohn's disease and rheumatoid arthritis: results of a systematic review
- PMID: 23885145
- PMCID: PMC3718902
- DOI: 10.3748/wjg.v19.i27.4344
Low rates of adherence for tumor necrosis factor-α inhibitors in Crohn's disease and rheumatoid arthritis: results of a systematic review
Abstract
Aim: To investigate adherence rates in tumor necrosis factor-α (TNF-α)-inhibitors in Crohn's disease (CD) and rheumatoid arthritis (RA) by systematic review of medical literature.
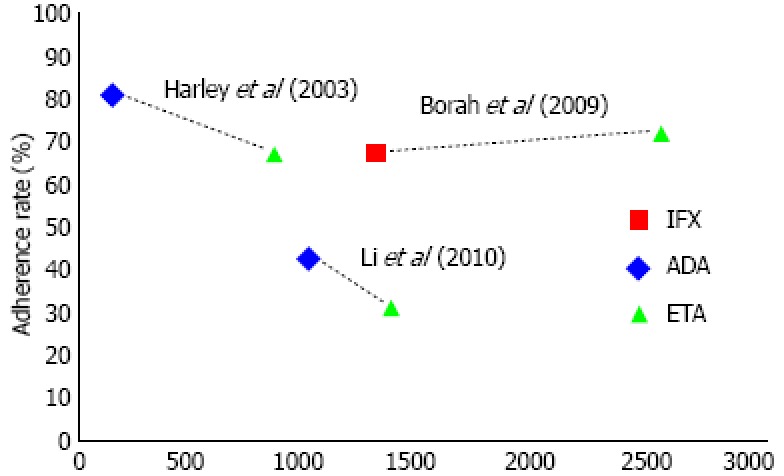
Methods: A structured search of PubMed between 2001 and 2011 was conducted to identify publications that assessed treatment with TNF-α inhibitors providing data about adherence in CD and RA. Therapeutic agents of interest where adalimumab, infliximab and etanercept, since these are most commonly used for both diseases. Studies assessing only drug survival or continuation rates were excluded. Data describing adherence with TNF-α inhibitors were extracted for each selected study. Given the large variation between definitions of measurement of adherence, the definitions as used by the authors where used in our calculations. Data were tabulated and also presented descriptively. Sample size-weighted pooled proportions of patients adherent to therapy and their 95%CI were calculated. To compare adherence between infliximab, adalimumab and etanercept, the adherence rates where graphed alongside two axes. Possible determinants of adherence were extracted from the selected studies and tabulated using the presented OR.
Results: Three studies on CD and three on RA were identified, involving a total of 8147 patients (953 CD and 7194 RA). We identified considerable variation in the definitions and methodologies of measuring adherence between studies. The calculated overall sample size-weighted pooled proportion for adherence to TNF-α inhibitors in CD was 70% (95%CI: 67%-73%) and 59% in RA (95%CI: 58%-60%). In CD the adherence rate for infliximab (72%) was highercompared to adalimumab (55%), with a relative risk of 1.61 (95%CI: 1.27-2.03), whereas in RA adherence for adalimumab (67%) was higher compared to both infliximab (48%) and etanercept (59%), with a relative risk of 1.41 (95%CI: 1.3-1.52) and 1.13 (95%CI: 1.10-1.18) respectively. In comparative studies in RA adherence to infliximab was better than etanercept and etanercept did better than adalimumab. In three studies, the most consistent factor associated with lower adherence was female gender. Results for age, immunomodulator use and prior TNF-α inhibitors use were conflicting.
Conclusion: One-third of both CD and RA patients treated with TNF-α inhibitors are non-adherent. Female gender was consistently identified as a negative determinant of adherence.
Keywords: Adherence; Crohn’s disease; Rheumatoid arthritis; Systematic review; Tumor necrosis factor-α inhibitors.
Figures


References
-
- Furst DE, Keystone EC, Braun J, Breedveld FC, Burmester GR, De Benedetti F, Dörner T, Emery P, Fleischmann R, Gibofsky A, et al. Updated consensus statement on biological agents for the treatment of rheumatic diseases, 2011. Ann Rheum Dis. 2012;71 Suppl 2:i2–45. - PubMed
-
- Ford AC, Sandborn WJ, Khan KJ, Hanauer SB, Talley NJ, Moayyedi P. Efficacy of biological therapies in inflammatory bowel disease: systematic review and meta-analysis. Am J Gastroenterol. 2011;106:644–659, quiz 660. - PubMed
-
- Ben-Horin S, Chowers Y. Review article: loss of response to anti-TNF treatments in Crohn’s disease. Aliment Pharmacol Ther. 2011;33:987–995. - PubMed
-
- Fernández-Nebro A, Irigoyen MV, Ureña I, Belmonte-López MA, Coret V, Jiménez-Núñez FG, Díaz-Cordovés G, López-Lasanta MA, Ponce A, Rodríguez-Pérez M, et al. Effectiveness, predictive response factors, and safety of anti-tumor necrosis factor (TNF) therapies in anti-TNF-naive rheumatoid arthritis. J Rheumatol. 2007;34:2334–2342. - PubMed
-
- Jackson CA, Clatworthy J, Robinson A, Horne R. Factors associated with non-adherence to oral medication for inflammatory bowel disease: a systematic review. Am J Gastroenterol. 2010;105:525–539. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
