

A new pancreaticojejunostomy technique: a battle against postoperative pancreatic fistula
- PMID: 23885146
- PMCID: PMC3718903
- DOI: 10.3748/wjg.v19.i27.4351
A new pancreaticojejunostomy technique: a battle against postoperative pancreatic fistula
Abstract
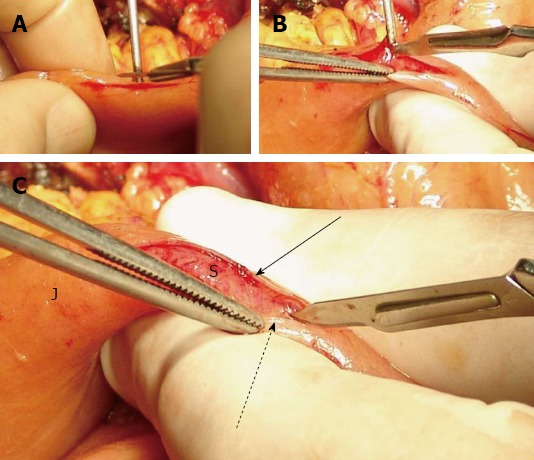
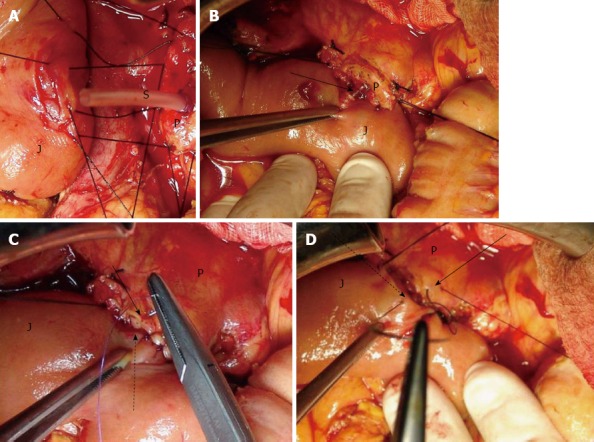
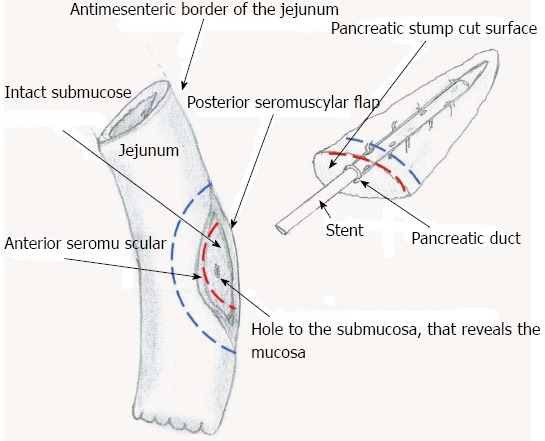
Aim: To present a new technique of end-to-side, duct-to-mucosa pancreaticojejunostomy with seromuscular jejunal flap formation, and insertion of a silicone stent.
Methods: We present an end-to-side, duct-to-mucosa pancreaticojejunostomy with seromuscular jejunal flap formation, and the insertion of a silicone stent. This technique was performed in thirty-two consecutive patients who underwent a pancreaticoduodenectomy procedure by the same surgical team, from January 2005 to March 2011. The surgical procedure performed in all cases was classic pancreaticoduodenectomy, without preservation of the pylorus. The diagnosis of pancreatic leakage was defined as a drain output of any measurable volume of fluid on or after postoperative day 3 with an amylase concentration greater than three times the serum amylase activity.
Results: There were 32 patients who underwent end-to-side, duct-to-mucosa pancreaticojejunostomy with seromuscular jejunal flap formation. Thirteen of them were women and 19 were men. These data correspond to 40.6% and 59.4%, respectively. The mean age was 64.2 years, ranging from 55 to 82 years. The mean operative time was 310.2 ± 40.0 min, and was defined as the time period from the intubation up to the extubation of the patient. Also, the mean time needed to perform the pancreaticojejunostomy was 22.7 min, ranging from 18 to 25 min. Postoperatively, one patient developed a low output pancreatic fistula, three patients developed surgical site infection, and one patient developed pneumonia. The rate of overall morbidity was 15.6%. There was no 30-d postoperative mortality.
Conclusion: This modification appears to be a significantly safe approach to the pancreaticojejunostomy without adversely affecting operative time.
Keywords: Pancreatic fistula; Pancreaticojejunostomy; Seromuscular jejunal flap; Technique; Whipple.
Figures
References
-
- Abu Hilal M, Malik HZ, Hamilton-Burke W, Verbeke C, Menon KV. Modified Cattell’s pancreaticojejunostomy, buttressing for soft pancreases and an isolated biliopancreatic loop are safety measurements that improve outcome after pancreaticoduodenectomy: a pilot study. HPB (Oxford) 2009;11:154–160. - PMC - PubMed
-
- Kausch W. Das Carcinoma der Papilla Duodeni und seine Vadikale Entfernung. Bietrage zur Klinischen Chirugen. 1912;78:439–486.
-
- Poon RT, Lo SH, Fong D, Fan ST, Wong J. Prevention of pancreatic anastomotic leakage after pancreaticoduodenectomy. Am J Surg. 2002;183:42–52. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
