

Physical therapy interventions for degenerative lumbar spinal stenosis: a systematic review
- PMID: 23886845
- PMCID: PMC3870489
- DOI: 10.2522/ptj.20120379
Physical therapy interventions for degenerative lumbar spinal stenosis: a systematic review
Abstract
Background: Physical therapy is commonly prescribed for patients with lumbar spinal stenosis (LSS); however, little is known about its effectiveness.
Purpose: The purpose of this study was to systematically review randomized controlled trials (RCTs), controlled trials, and cohort studies evaluating the effectiveness of physical therapy for LSS.
Data sources: Studies were searched on electronic databases to January 2012.
Study selection: Inclusion criteria were: clinical diagnosis of LSS with confirmatory imaging, evaluation of physical therapy treatment, presence of a comparison group, and outcomes of pain, disability, function, or quality of life.
Data extraction: Outcomes were extracted and, when possible, pooled using RevMan 5, a freely available review program from the Cochrane Library.
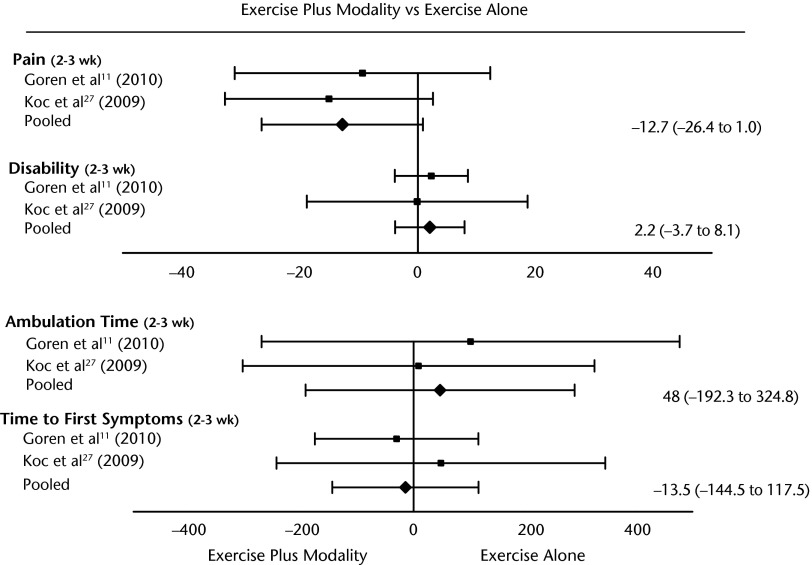
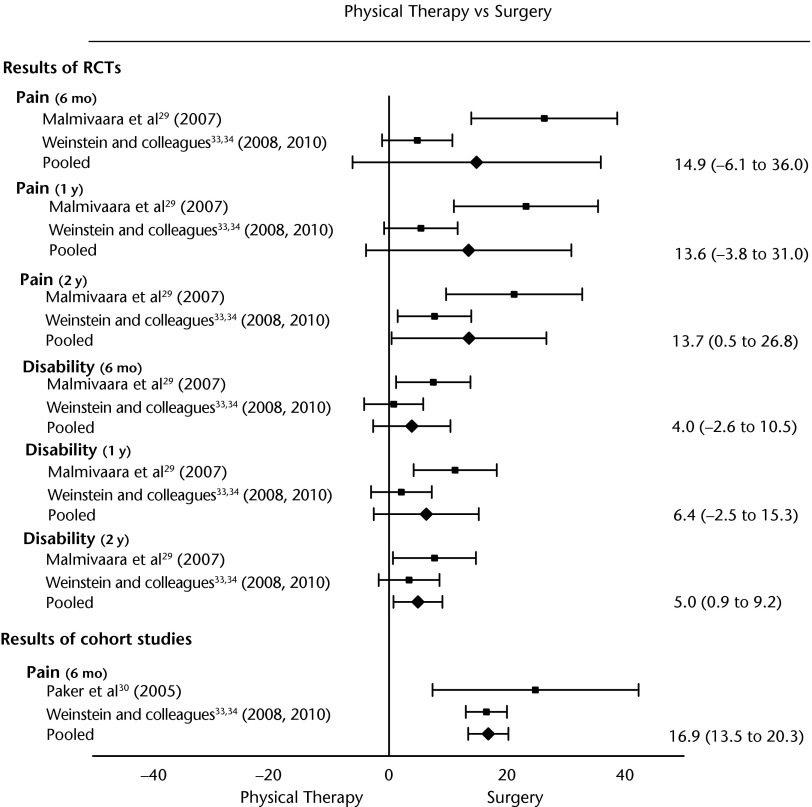
Data synthesis: Ten studies were included: 5 RCTs, 2 controlled trials, 2 mixed-design studies, and 1 longitudinal cohort study. Pooled effects of 2 studies revealed that the addition of a physical therapy modality to exercise had no statistically significant effect on outcome. Pooled effects results of RCTs evaluating surgery versus physical therapy demonstrated that surgery was better than physical therapy for pain and disability at long term (2 years) only. Other results suggested that exercise is significantly better than no exercise, that cycling and body-weight-supported treadmill walking have similar effects, and that corsets are better than no corsets.
Limitations: The limitations of this review include the low quality and small number of studies, as well as the heterogeneity in outcomes and treatments.
Conclusions: No conclusions could be drawn from the review regarding which physical therapy treatment is superior for LSS. There was low-quality evidence suggesting that modalities have no additional effect to exercise and that surgery leads to better long-term (2 years) outcomes for pain and disability, but not walking distance, than physical therapy in patients with LSS.
Figures

References
-
- Haig AJ, Tong HC, Yamakawa KSJ, et al. Spinal stenosis, back pain, or no symptoms at all? A masked study comparing radiologic and electrodiagnostic diagnosis to the clinical impression. Arch Phys Med Rehabil. 2006;87:897–903 - PubMed
-
- Jansson KA, Nemeth G, Granath F, et al. Health-related quality of life (EQ-5D) before and one year after surgery for lumbar spinal stenosis. J Bone Joint Surg Br. 2009;91:210–216 - PubMed
-
- Atlas SJ, Keller RB, Wu YA, et al. Long-term outcomes of surgical and nonsurgical management of lumbar spinal stenosis: 8 to 10 year results from the Maine Lumbar Spine Study. Spine (Phila Pa 1976). 2005;30:936–943 - PubMed
-
- Fritz JM, Erhard RE, Delitto A, et al. Preliminary results of the use of a two-stage treadmill test as a clinical diagnostic tool in the differential diagnosis of lumbar spinal stenosis. J Spinal Disord. 1997;10:410–416 - PubMed
-
- Kapural L, Mekhail N, Bena J, et al. Value of the magnetic resonance imaging in patients with painful lumbar spinal stenosis (LSS) undergoing lumbar epidural steroid injections. Clin J Pain. 2007;23:571–575 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
