

Current trends in preoperative biliary stenting in patients with pancreatic cancer
- PMID: 23889947
- PMCID: PMC3728700
- DOI: 10.1016/j.surg.2013.03.016
Current trends in preoperative biliary stenting in patients with pancreatic cancer
Abstract
Background: Sufficient evidence suggests that preoperative biliary stenting is associated with increased complication rates after pancreaticoduodenectomy.
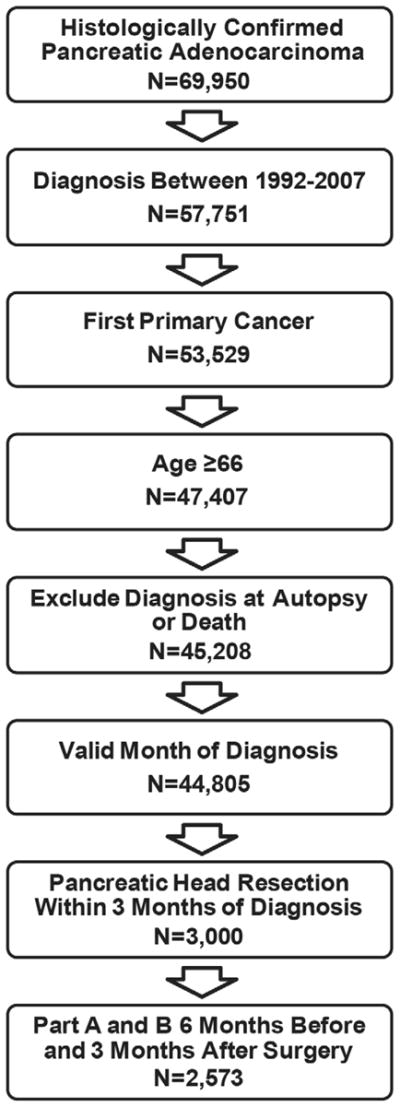
Methods: Surveillance, Epidemiology, and End Results (SEER) and linked Medicare claims data (1992-2007) were used to identify patients with pancreatic cancer who underwent pancreaticoduodenectomy. We evaluated trends in the use of preoperative biliary stenting, timing of physician visits relative to stenting, and time to surgical resection and symptoms in stented and unstented patients.
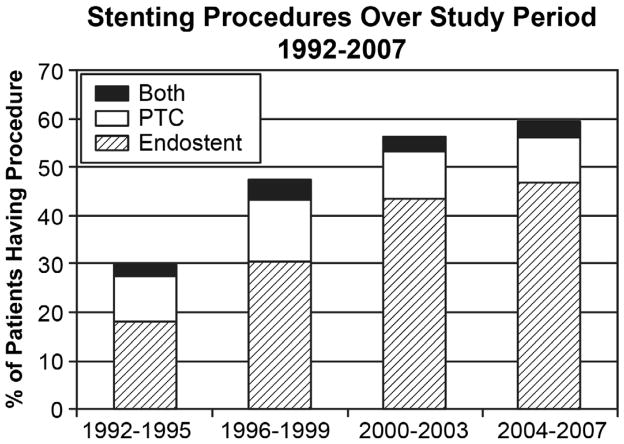
Results: Pancreaticoduodenectomy was performed in 2,573 patients, and 52.6% of patients underwent preoperative biliary stenting (N = 1,354). Of these, 75.3% underwent endoscopic stenting only, 18.9% received a percutaneous stent, and 5.8% underwent both procedures. The overall stenting rate increased from 29.6% of patients between 1992 and 1995 to 59.1% between 2004 and 2007 (P < .0001). Preoperative stenting was more common in patients with jaundice, cholangitis, pruritus, or coagulopathy (P < .05 for all). Of stented patients, 77.7% had had a stent placed prior to seeing a surgeon. Stenting prior to surgical consultation was associated with longer indwelling stent time compared to stenting after surgical consultation (37.3 vs 27.0 days, P < .0001). In addition, stented patients had longer times from surgeon visit to pancreatectomy than those who had not received stents (24.2 days vs 17.2 days, P < .0001).
Conclusion: Use of preoperative biliary stenting doubled between 1992 and 2007 despite evidence that stenting is associated with increased perioperative infectious complications. The majority of stenting occurred prior to surgical consultation and is associated with significant delay in time to operation. Surgeons should be involved early in order to prevent unnecessary stenting and improve outcomes.
Copyright © 2013 Mosby, Inc. All rights reserved.
Figures
References
-
- Denning DA, Ellison EC, Carey LC. Preoperative percutaneous transhepatic biliary decompression lowers operative morbidity in patients with obstructive jaundice. Am J Surg. 1981;141(1):61–5. - PubMed
-
- Gundry SR, Strodel WE, Knol JA, et al. Efficacy of preoperative biliary tract decompression in patients with obstructive jaundice. Arch Surg. 1984;119(6):703–8. - PubMed
-
- Lygidakis NJ, van der Heyde MN, Lubbers MJ. Evaluation of preoperative biliary drainage in the surgical management of pancreatic head carcinoma. Acta Chir Scand. 1987;153(11–12):665–8. - PubMed
-
- Smith RC, Pooley M, George CR, et al. Preoperative percutaneous transhepatic internal drainage in obstructive jaundice: a randomized, controlled trial examining renal function. Surgery. 1985;97(6):641–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
